- Protocols

- Articles and Issues
- For Authors
- About
- Become a Reviewer

Detection of Autophagy in Human Peripheral Blood Mononuclear Cells Using Guava® Autophagy and Flow Cytometry
(*contributed equally to this work) Published: Vol 15, Iss 18, Sep 20, 2025 DOI: 10.21769/BioProtoc.5457 Views: 1606
Reviewed by: Anonymous reviewer(s)
Original research article
The authors used this protocol in:

Feb 2024
Advertisement

Protocol Collections
Comprehensive collections of detailed, peer-reviewed protocols focusing on specific topics






Related protocols

Abstract
Autophagy plays a crucial role in cellular homeostasis and is responsible for removing and degrading damaged cytoplasmic cargo. This lysosome-mediated catabolic process removes defective organelles and misfolded proteins, and impaired autophagy has been directly linked to ageing and numerous diseases. This emphasises the importance of developing intervention methods to counteract this dysregulation. One promising intervention is thermal therapy, specifically hyperthermia, which is described in this protocol. In order to investigate this form of treatment, a rapid and reliable detection method is required to allow comparison of autophagy status under different conditions. While methods such as transmission electron microscopy (TEM) or western blotting can provide valuable structural analysis, they are often time-consuming and expensive, and are not suitable for small, round cells such as peripheral blood mononuclear cells (PBMCs). The method described in this protocol enables absolute quantification of PBMCs using the Guava® Autophagy Detection kit after heat treatment with water-filtered infrared-A radiation (wIRA), compared with an untreated control. This method is based on antibody labelling, and subsequent flow cytometric analysis enables the number of autophagosomes to be determined by measuring the FITC intensity. This protocol provides rapid, reliable results and can be adapted to investigate not only heat therapy, but also other interventions, such as caloric restriction.
Key features
• Rapid and reliable ex vivo quantification of autophagy in living cells.
• Optimised protocol for the determination of autophagy in primary human blood cells.
• Allows the testing of active substances and treatments concerning autophagy.
• Flow cytometry–based method for the determination of autophagy.
Keywords: Human peripheral blood mononuclear cells (PBMCs)Graphical overview
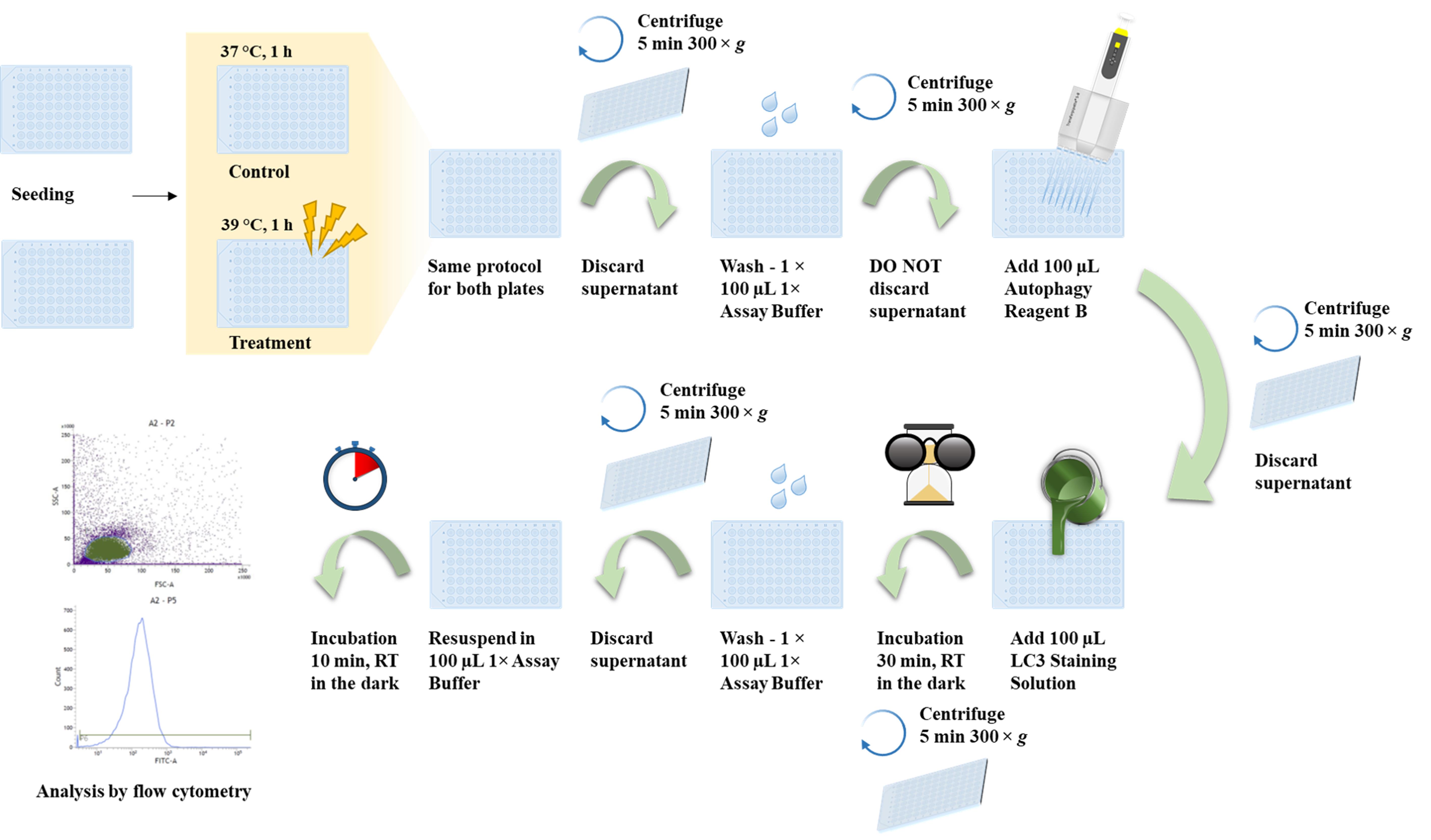
Autophagy detection in human peripheral blood mononuclear cells (PBMCs) using the Guava® Autophagy Detection kit
Background
The highly selective, lysosome-dependent catabolic pathway of autophagy is part of normal cellular housekeeping as well as cellular homeostasis. This highly conserved process is responsible for the removal and recycling of damaged cytoplasmic cargo, such as defective organelles or misfolded proteins in the form of aggregates. The core autophagic process involves the formation of double-membrane vesicles, called autophagosomes, that engulf the cytoplasmic cargo and then fuse with the lysosome. After fusion, lysosomal hydrolases are responsible for the degradation (see Figure 1) [1].
Impaired autophagy has been associated with ageing as well as a multitude of different diseases and pathologies, including cancer and neurodegenerative diseases such as Alzheimer’s, Parkinson’s, or Huntington’s disease, among others [1,2]. This illustrates the need to counteract impaired autophagy and to explore the possibility of inducing autophagy through treatment options or supplementation with substances. Known autophagy inducers are cellular stress, for example, in the form of caloric restriction or exercise. Further, autophagy is shown to be induced by hypoxia, DNA damage, ER stress, and microbial pathogen infection [3,4]. Heat stress is also a known inducer of autophagy [5], which, in this protocol, can be administered in the form of hyperthermia. This hyperthermia, also known as thermal therapy or heat treatment, uses a specialised heat source in the form of water-filtered infrared-A radiation (wIRA) with a wavelength ranging from 780 to 1,400 nm. For the warming of the whole body, the IRATHERM®1000M (Von Ardenne Institute of Applied Medical Research GmbH, Dresden, Germany) is used. To heat isolated human primary peripheral blood mononuclear cells (PBMCs), a portable device called IRAcubator with the same heat source is utilised. This is only one example of a treatment method that modulates autophagy, but it demonstrates the need for a reliable and reproducible method. This is particularly important for small, round cells such as PBMCs, which have a high nucleus-to-cytoplasm ratio and for which classic methods of localising and quantifying autophagosomes are ineffective. Prominent methods for autophagy monitoring are transmission electron microscopy (TEM), western blotting, or the use of reporter systems [6]. Besides being very time-consuming and expensive, TEM is rather suited for structural and qualitative analysis as opposed to quantitative analysis. Nevertheless, TEM remains one of the gold standards in autophagy detection, but it is limited to non-living cells. Western blotting requires vast amounts of sample material, making it unsuitable for studies where the sample material is scarce. Further, it is also very time-consuming and expensive. Reporter systems are elegant methods when working with cell lines, but are not feasible when working with primary cells from in vivo treatments.
Other methods, such as CYTO-ID®, are fast, reliable, and relatively cost-effective, but have severe limitations in small and round cells like PBMCs, as discussed in our previous work [7].
The Guava® Autophagy Detection kit used in this protocol contains a FITC-labelled anti-LC3 antibody. By optimising the cell number and incubation steps, an ideal staining for PBMCs can be achieved. In addition, the lysosomal inhibitor chloroquine can be used as a positive control. By inhibiting the fusion of the lysosome to the autophagosome, the autophagic process is interrupted, leading to the accumulation of autophagosomes (Figure 1). Therefore, wells that contain chloroquine should show a higher median fluorescent intensity (MFI) if staining has worked properly. For both conditions, additional wells containing chloroquine are prepared as a positive control.
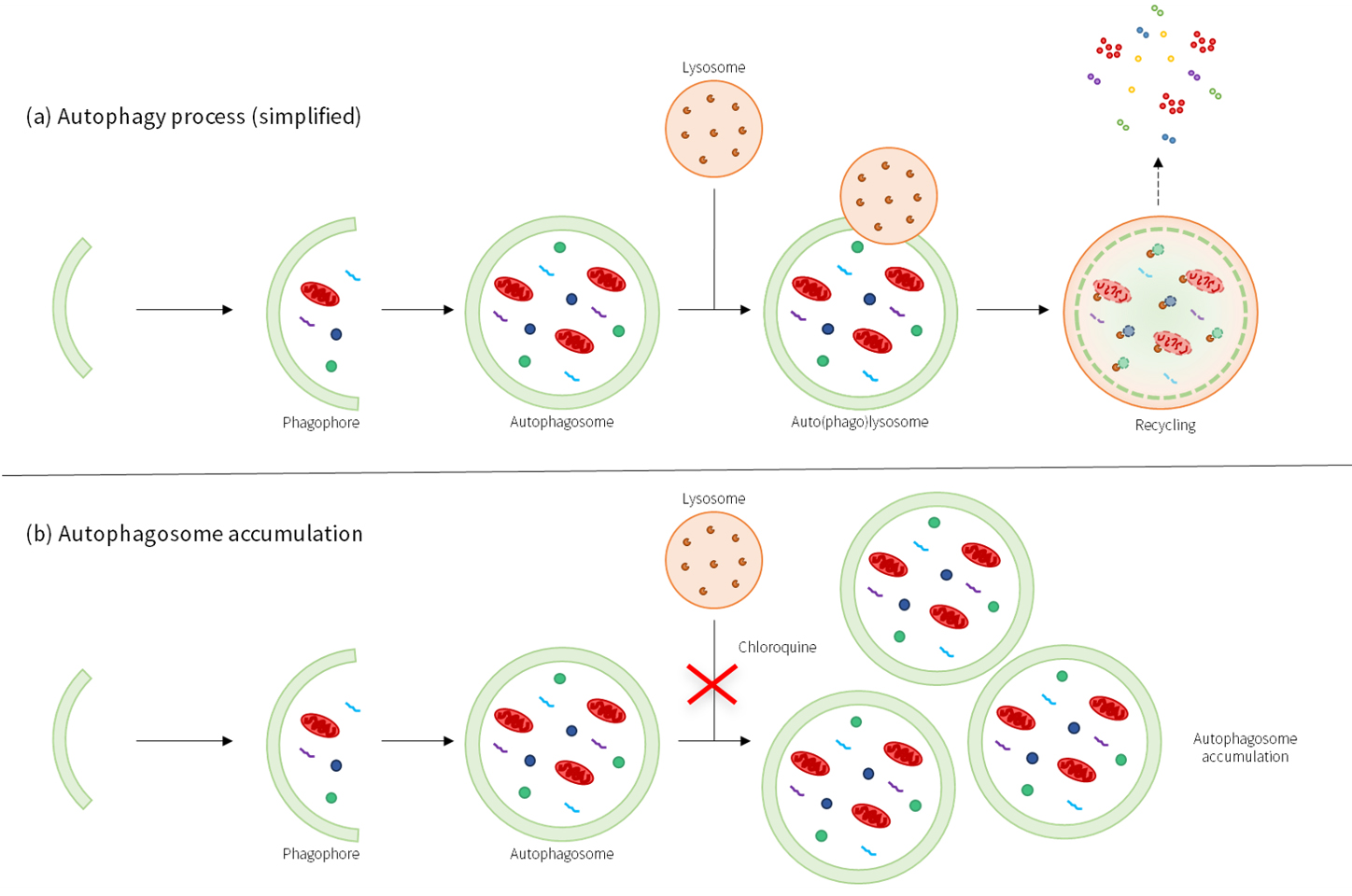
Figure 1. Schematic overview of the autophagy process under different conditions. Under normal conditions, the mature autophagosome fuses with the lysosome, resulting in the degradation of the vesicles (a). In the presence of chloroquine, however, the fusion is inhibited, resulting in accumulation of the autophagosomes (b).
This method proved to be rapid, reliable, and cost-effective. Moreover, it can not only be used to investigate the effects of hyperthermia but can also be adapted to investigate a multitude of treatments and therapies in vivo and ex vivo.
Materials and reagents
Biological materials
1. Primary human peripheral blood mononuclear cells (PBMCs) from volunteers
Reagents
1. S-Monovette® K3 EDTA 9 mL (SARSTEDT, catalog numbers: 02.1066.001)
2. Ficoll-PaqueTM PLUS density gradient media (Cytiva, catalog number: 17-1440-03)
3. RPMI medium 1640 (1×) without phenol red (GibcoTM, catalog number: 11835063)
4. Chloroquine diphosphate (TOCRIS, catalog number: 4109)
5. Dimethyl sulphoxide (DMSO) ≥ 99.5%, BioScience grade (Carl Roth, catalog number: A994.2)
5. Guava® Autophagy LC3 Antibody-Based Detection kit (Cytek®, catalog number: FCCH100171)
6. Sodium chloride (NaCl) (Carl Roth, catalog number: 3957)
7. Di-sodium hydrogen phosphate dodecahydrate (Na2HPO4·12H2O) (Carl Roth, catalog number: N350)
8. Potassium dihydrogen phosphate (KH2PO4) (Carl Roth, catalog number: 3904)
9. Potassium chloride (KCl) (Carl Roth, catalog number: 6781)
10. Water, molecular biology grade (VWR, catalog number: VWRL0201-0500)
11. Acridine orange/propidium iodide stain (Logos, catalog number: F23001)
Solutions
1. Physiological saline solution (0.9% NaCl) (see Recipes)
2. 1× Phosphate buffered saline (PBS) (see Recipes)
3. 1× Assay buffer (see Recipes)
4. Autophagy reagent B (see Recipes)
5. LC3 staining solution (see Recipes)
Recipes
1. Physiological saline solution (0.9% NaCl)
| Reagent | Final concentration | Quantity or volume |
|---|---|---|
| NaCl | 0.9% (w/v) | 9.0 g |
| Deionized water | n/a | to 1,000 mL |
| Total | n/a | 1,000 mL |
Autoclave and store at room temperature.
2. 1× PBS
| Reagent | Final concentration | Quantity or volume |
|---|---|---|
| NaCl | 8.0% (w/v) | 80.0 g |
| KCl | 0.2% (w/v) | 2.0 g |
| Na2HPO4·12H2O | 1.78% (w/v) | 17.8 g |
| KH2PO4 | 0.24% (w/v) | 2.4 g |
| Deionized water | n/a | to 1,000 mL |
| Total | n/a | 1,000 mL |
Adjust pH value to 7.4. Autoclave 10× PBS; for 1× PBS, dilute 10× stock 1:10 with deionized water (50 mL of 10× PBS + 450 mL of deionized water), autoclave, and store at room temperature.
3. 1× Assay buffer
| Reagent | Final concentration | Quantity or volume |
|---|---|---|
| 5× Assay buffer (from Guava®) | 1× | 55 mL |
| Deionized water | n/a | 220 mL |
| Total | n/a | 275 mL |
Dilute and then sterilize by filtration and store at 4 °C for up to one year.
4. Autophagy reagent B
| Reagent | Final concentration | Quantity or volume |
|---|---|---|
| Autophagy reagent B (10×) | 1× | 1 mL |
| Water, molecular biology grade | n/a | 9 mL |
| Total | n/a | 10 mL |
Aliquot and store at 4 °C for up to one year.
5. LC3 staining solution
| Reagent | Final concentration | Quantity or volume |
|---|---|---|
| 20× anti-LC3/FITC antibody | 1× | 62.5 µL |
| 1× assay buffer | n/a | 1,187.5 µL |
| Total | n/a | 1,250.0 µL |
Prepare immediately before use; do not store. Protect from light. All listed ingredients are part of the Guava® Autophagy LC3 Antibody-Based Detection kit.
Laboratory supplies
1. LeucosepTM with porous barrier, 50 mL (Greiner Bio-One GmbH, catalog number: 227290)
2. Centrifuge tubes, 15 and 50 mL (SARSTEDT, catalog numbers: 62.554.502, 62.547.254)
3. Reaction tubes, 1.5 and 2 mL (SARSTEDT, catalog numbers: 72.706, 72.695.500)
4. LUNA 2-channel cell counting slides (Logos, catalog number: L12002-LG)
5. Pipette tips, 20, 200, and 1,000 μL (SARSTEDT, catalog numbers: 701.114.210, 70.3030, and 70.3050)
6. Serological pipettes, 5, 10, and 25 mL (SARSTEDT, catalog numbers: 86.1253.001, 86.1254.001, and 86.1685.001)
7. Syringe filter, Filtropur S, pore size: 0.2 μm (SARSTEDT, catalog number: 83.1826.001)
8. Corning® 96-well clear V-bottom TC-treated microplates (Corning, catalog number: 3894)
Equipment
1. Pipettes: Eppendorf Research® Plus 10 μL, 20 μL, 200 μL, 1,000 μL (Eppendorf, catalog numbers: 3123000020, 3123000039, 3123000055, 3123000063)
2. Multichannel microliter pipette Transferpette®, 20–200 µL (BRAND GMBH + CO.KG, catalog number: 9280173)
3. Pipetting aid: PipetBoy acu 2 (Integra Biosciences, catalog number: 155 000)
4. LunaTM fl Dual Fluorescence Cell Counter (Logos, model: L20001-LG)
5. Water bath (GFL, catalog number: 1003)
6. Microcentrifuge Eppendorf 5424 (Eppendorf, catalog number: 05-400-005)
7. Swing-out rotor centrifuge Eppendorf 5804 R (Eppendorf, catalog numbers: 5805000010, 5804709004)
8. Water purification system ELGA® PURELAB flex 3 (Veolia, catalog number: PF3XXXXM1)
9. pH meter FE20 FiveEasyTM (Mettler Toledo, catalog number: 30266626)
10. Heat treatment IRAcubator (Von Ardenne Institut für Angewandte Medizinische Forschung GmbH)
11. Incubator at 37 °C with 5% CO2, 90% humidity (HERA Cell 240, catalog number: 2510-413-01)
12. BD FACSVerseTM with 488 nm laser (BD Biosciences, catalog number: 651155)
Software and datasets
1. BD FACSSuite (BD Biosciences, v1.0.6), license needed
2. GraphPad Prism (GraphPad Software, Inc., v. 10.4.2), license needed
Procedure
A. PBMC isolation
1. Warm the Ficoll-PaqueTM PLUS separation medium to room temperature (RT), protected from light, and fill the LeucosepTM tube with 15 mL separation medium. Centrifuge at 1,000× g for 1 min at RT. The separation medium is now located below the porous barrier.
Note: All centrifugation steps are carried out at RT.
2. Dilute an appropriate volume of anticoagulated human blood (collected in 9 mL of K3 EDTA S-Monovette®) at a ratio of 1:2 with 0.9% NaCl solution in a separate centrifuge tube. Transfer the diluted blood carefully into the prepared LeucosepTM tube (at least 15 mL and at most 30 mL).
3. Centrifuge at 1,000× g for 10 min in a swing-out rotor with brake switched off.
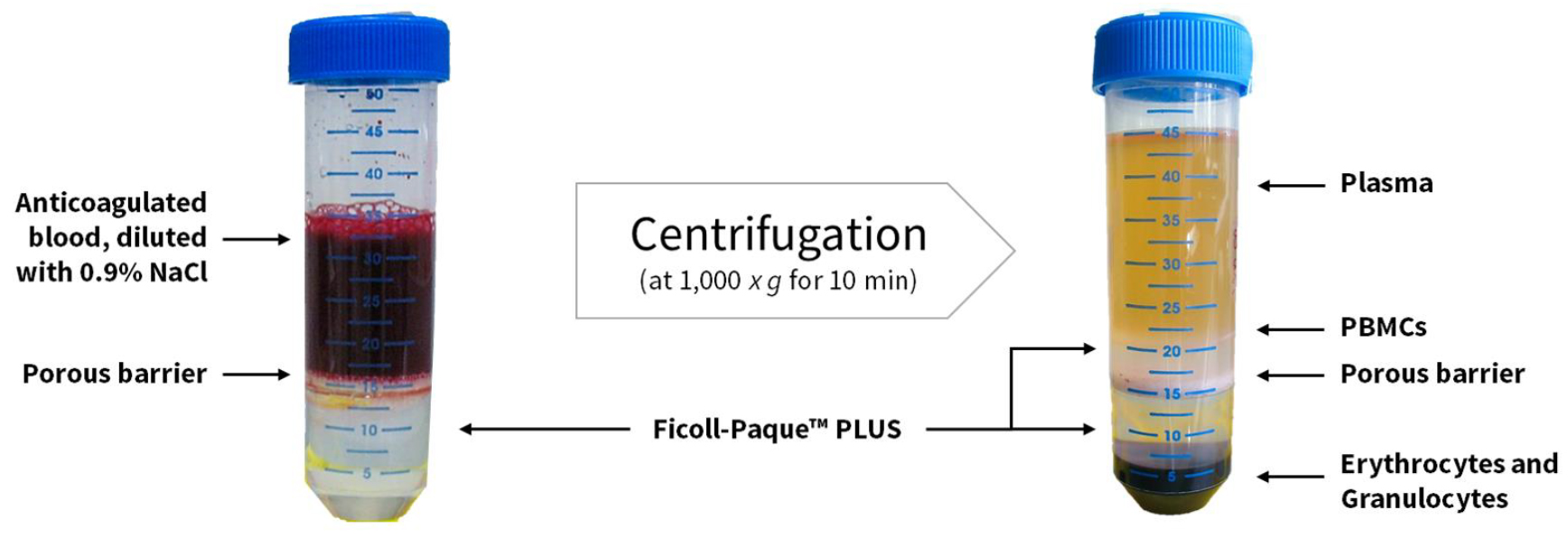
Figure 2. Primary human peripheral blood mononuclear cell (PBMC) isolation using LeucosepTM tubes. On the left side, the porous barrier separates the Ficoll-PaqueTM PLUS (bottom) and the diluted anticoagulated blood (top). On the right side, after centrifugation, the sequence of layers occurs as follows (from top to bottom): plasma > enriched cell fraction (PBMCs) > Ficoll-PaqueTM PLUS > porous barrier > Ficoll-PaqueTM PLUS > erythrocytes and granulocytes.
4. Collect and discard approximately 10 mL of plasma from the top (Figure 2), leaving a minimum remnant of 5–10 mm above the interphase, to prevent contamination of the enriched cells with platelets and facilitate harvesting of the enriched cell fraction.
5. Harvest the enriched cell fraction (lymphocytes/PBMCs) using a 1,000 μL Eppendorf pipette. The porous barrier effectively prevents recontamination with pelleted erythrocytes and granulocytes (for detailed information, see the manufacturer's instructions or refer to [8]).
6. Wash the cells with 15 mL of 1× PBS and subsequently centrifuge at 250× g for 10 min with the brake switched back on.
7. Repeat the washing step twice, resuspending the cell pellet in 10 mL of PBS each time.
8. Determine the cell count using acridine orange/propidium iodide stain and the LunaTM fl Dual Fluorescence Cell Counter.
B. Cell seeding and treatment
1. Prepare six wells per plate (control plate, treatment plate) with 500,000 cells/well in a 96-well plate (V-bottom) in 200 μL of RPMI medium (Figure 3a.) or 200 μL of RPMI medium with 40 μM chloroquine (CQ; diluted with RPMI medium from 600 µM CQ in DMSO) (Figure 3b.) in triplicate (Figure 3).
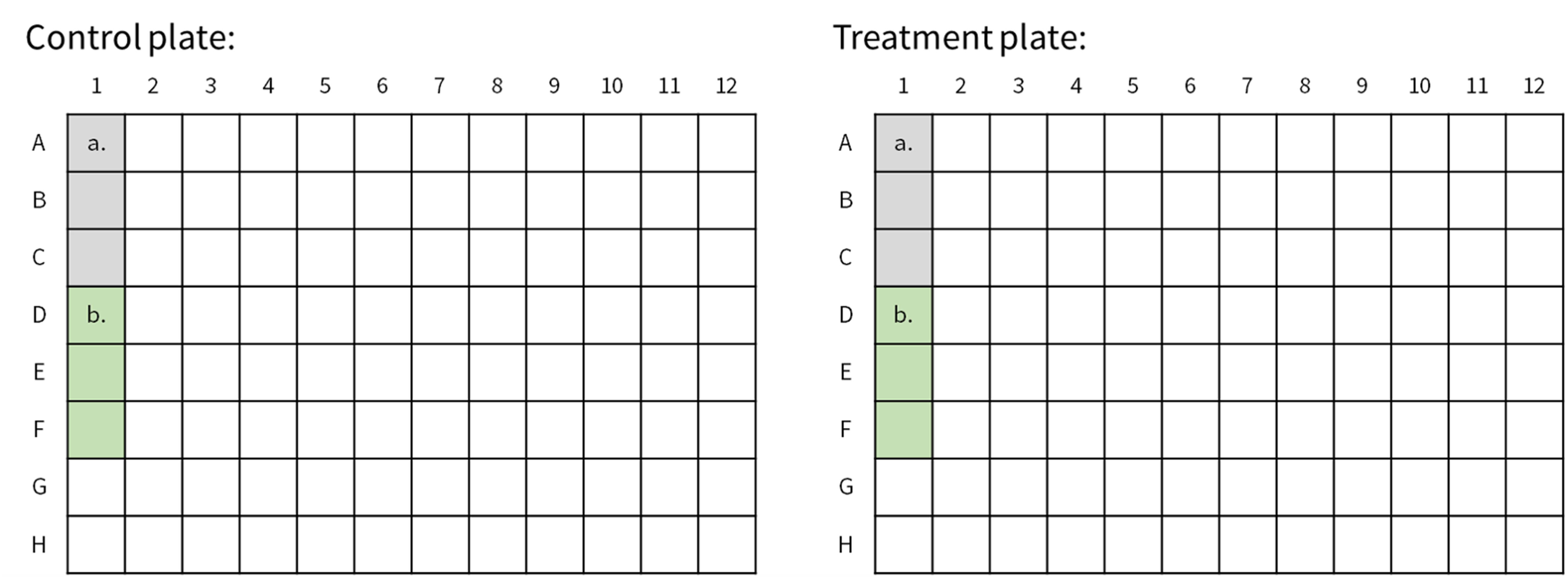
Figure 3. Plate layouts. Both the control plate (left) and the treatment plate (right) contain three wells with RPMI medium (a.) for measurement and six wells with RPMI medium with 40 µM chloroquine (b.) as a positive control.
2. The IRAcubator should be preheated to 39 °C.
3. Place the control plate in a humidified incubator at 37 °C and 5% CO2 for 1 h.
4. Place the treatment plate in the IRAcubator at 39 °C for 1 h (Figure 3) (for detailed information, refer to [7]).
C. Guava® autophagy detection
1. After incubation with CQ and/or treatment, centrifuge the plates at 300× g for 5 min. Discard the supernatant by turning the plate(s) over onto laboratory tissue paper.
2. Resuspend the pellets in 100 μL of 1× assay buffer, then centrifuge the plates again at 300× g for 5 min.
Note: Allow all assay components to reach RT.
3. After centrifugation, add 100 μL of autophagy reagent B directly to each well, then immediately centrifuge again at 300× g for 5 min.
Caution: Do not discard the supernatant; otherwise, the concentration of autophagy reagent B will be incorrect.
4. Discard the supernatant by turning the plate(s) over onto laboratory tissue paper. Resuspend the pellets in 100 μL of LC3 staining solution and leave to incubate for 30 min at RT in the dark.
Note: All subsequent steps are carried out in the dark.
5. After incubation, centrifuge at 300× g for 5 min and discard the supernatant by turning the plate(s) over onto laboratory tissue paper.
6. Wash the samples once with 100 μL of 1× assay buffer to remove any residual or unbound antibody.
7. Centrifuge at 300× g for 5 min and discard the supernatant by turning the plate(s) over onto laboratory tissue paper.
8. Resuspend the pellets in 100 μL of 1× assay buffer and then leave the plates for 10 min at RT in the dark, directly before measurement.
9. Analyse samples via flow cytometry with BD FACSVerseTM for data acquisition.
D. Data acquisition
1. The analysis of antibody-based LC3 detection is carried out via flow cytometry using a BD FACSVerseTM instrument. Samples are measured directly in 96-well plates using a universal loader.
Caution: Make sure to use the right plate geometry (Corning® standard conical bottom).
2. After manually gating the lymphocytes using forward scatter (FSC) and side scatter (SSC), the median fluorescence intensity (MFI) is measured (Figure 4).
3. A total of 10,000 events are gated, and the FITC-A median is defined as the MFI and used for subsequent analysis.
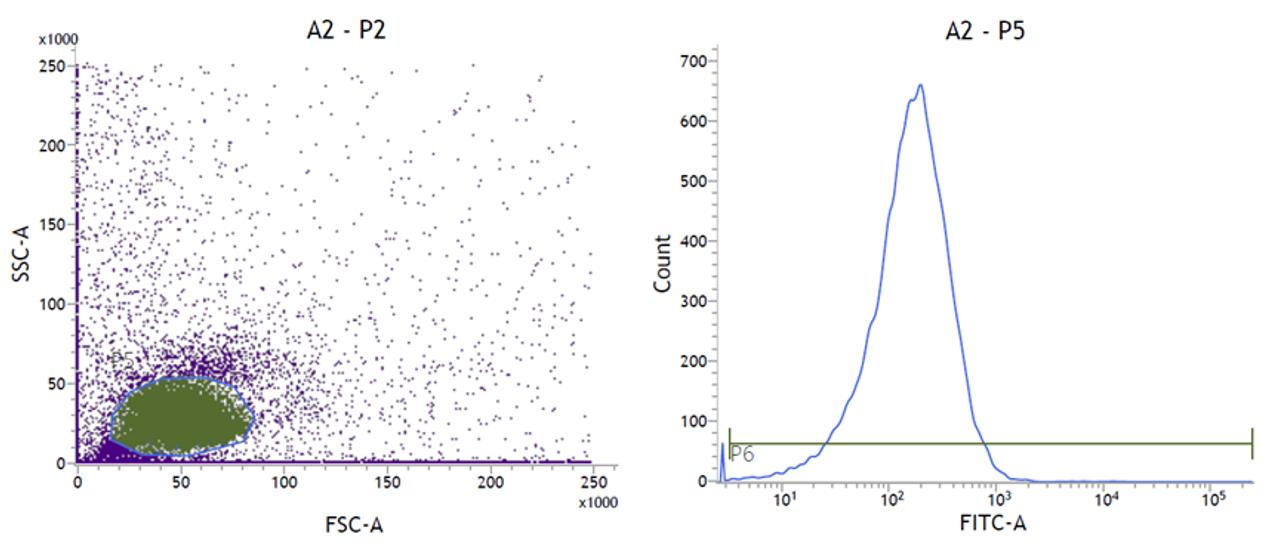
Figure 4. Forward scatter/side scatter (FSC/SSC) and histogram plots for the gating process (LC3 detection). As only a subpopulation (lymphocytes) of the total measured cells is relevant for LC3 detection, the corresponding population is manually gated in the FSC and SSC plots (left). Based on this population, the number of FITC-positive events is measured in the histogram (right).
Data analysis
As previously stated, three technical replicates should be carried out for each condition. Outliers can be excluded; we recommend defining them as the mean plus/minus three standard deviations.
Statistical analyses can be performed using any version of Prism (GraphPad Software, Inc.) or your preferred statistical software (e.g., R).
Validation of protocol
This protocol (or parts of it) has been used and validated in the following research articles:
Hochecker et al. [9] Heat treatment in health and disease: How water-filtered infrared-A (wIRA) irradiation affects key cellular mechanisms in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) patients compared to healthy donors. Journal of Thermal Biology (Figure 2).
Hochecker et al. [10] Heat vs. Fatigue: Hyperthermia as a Possible Treatment Option for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). International Journal of Molecular Sciences (Figure 1).
General notes and troubleshooting
General notes
1. When investigating the direct effect of an intervention on the organism (see [10]), the “before” and “after” measurements must be carried out directly, meaning there should be no delay between the two samples, and the samples must be measured independently, even if this means the measurements are taken on different days.
Troubleshooting
Problem 1: The 10× assay buffer shows signs of precipitation.
Possible cause: The 10× assay buffer was stored at too low a temperature.
Solution: Place the bottle in a 37 °C water bath, shaking or swirling occasionally. If the precipitate does not completely dissolve, leave the 10× assay buffer at RT overnight.
Problem 2: The lymphocyte population is outside of the predefined population gate.
Possible cause: Due to donor variability, the population has slightly shifted in the FSC/SSC plot.
Solution: Manually adjust the gate to encompass the entire lymphocyte population.
Problem 3: The CQ-treated cells show no offset in the histogram plot.
Possible cause: Either the concentration of CQ was not suitable for this cell type, or the incubation period was too short.
Solution: Determine the appropriate concentration of CQ via titration for the intended cell type or increase the incubation time with CQ prior to the assay.
Acknowledgments
Author contributions: Conceptualization, M.S., B.H., K.M., A.M., and J.B.; Investigation, M.S., B.H.; Writing—Original Draft, M.S.; Writing—Review & Editing, M.S., B.H., K.M., and J.B.; Funding acquisition, J.B.; Supervision, K.M., B.H., and J.B. The authors thank Dr Stefan Pieper and Dr Achim Schneider for providing the blood samples. The authors also thank Dr Alexander von Ardenne and Noah Molinski for the construction of the IRAcubator and good cooperation. This work was funded by the Professor Manfred von Ardenne Forschungsförderungsgesellschaft e.V. This work was also funded by the Baden-Württemberg Ministry for Science, Research and Art (MWK Baden-Württemberg) as part of the Kooperatives Promotionskolleg (KPK) InViTe2 Sigmaringen/Konstanz by financing Melanie Scherer as a doctoral student, and in which Barbara Hochecker is an associated PhD student. This protocol was used in Hochecker et al. [9] and Hochecker et al. [10].
Competing interests
The authors declare the following financial interests/personal relationships, which may be considered as potential competing interests: Melanie Scherer reports that financial support was provided by the MWK Baden-Württemberg. Barbara Hochecker reports that financial support was provided by Professor Manfred von Ardenne Forschungsförderungsgesellschaft e.V.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Landesärztekammer Baden-Württemberg (F-2013-066#A2, 31 January 2023). Informed consent was obtained from all subjects.
References
- Aman, Y., Schmauck-Medina, T., Hansen, M., Morimoto, R. I., Simon, A. K., Bjedov, I., Palikaras, K., Simonsen, A., Johansen, T., Tavernarakis, N., et al. (2021). Autophagy in healthy aging and disease. Nat Aging. 1(8): 634–650. https://doi.org/10.1038/s43587-021-00098-4
- Yang, Y. and Klionsky, D. J. (2020). Autophagy and disease: unanswered questions. Cell Death Differ. 27(3): 858–871. https://doi.org/10.1038/s41418-019-0480-9
- Kroemer, G., Mariño, G. and Levine, B. (2010). Autophagy and the Integrated Stress Response. Mol Cell. 40(2): 280–293. https://doi.org/10.1016/j.molcel.2010.09.023
- King, J. S., Veltman, D. M. and Insall, R. H. (2011). The induction of autophagy by mechanical stress. Autophagy. 7(12): 1490–1499. https://doi.org/10.4161/auto.7.12.17924
- McCormick, J. J., Dokladny, K., Moseley, P. L. and Kenny, G. P. (2021). Autophagy and heat: a potential role for heat therapy to improve autophagic function in health and disease. J Appl Physiol. 130(1): 1–9. https://doi.org/10.1152/japplphysiol.00542.2020
- Klionsky, D. J., Abdel-Aziz, A. K., Abdelfatah, S., Abdellatif, M., Abdoli, A., Abel, S., Abeliovich, H., Abildgaard, M. H., Abudu, Y. P., Acevedo-Arozena, A., et al. (2021). Guidelines for the use and interpretation of assays for monitoring autophagy (4th edition)1. Autophagy. 17(1): 1–382. https://doi.org/10.1080/15548627.2020.1797280
- Hochecker, B., Matt, K., Meßmer, A., Scherer, M. and Bergemann, J. (2024). Quantification of Autophagosomes in Human Fibroblasts Using Cyto-ID® Staining and Cytation Imaging. Bio Protoc. 14(1348): e5025. https://doi.org/10.21769/bioprotoc.5025
- Matt, K. and Bergemann, J. (2019). Ex vivo Analysis of DNA Repair Capacity of Human Peripheral Blood Mononuclear Cells by a Modified Host Cell Reactivation Assay. Bio Protoc. 9(15): e3325. https://doi.org/10.21769/bioprotoc.3325
- Hochecker, B., Molinski, N., Matt, K., Meßmer, A., Scherer, M., von Ardenne, A. and Bergemann, J. (2024). Heat treatment in health and disease: How water-filtered infrared-A (wIRA) irradiation affects key cellular mechanisms in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) patients compared to healthy donors. J Therm Biol. 120: 103813. https://doi.org/10.1016/j.jtherbio.2024.103813
- Hochecker, B., Matt, K., Scherer, M., Meßmer, A., von Ardenne, A. and Bergemann, J. (2025). Heat vs. Fatigue: Hyperthermia as a Possible Treatment Option for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Int J Mol Sci. 26(11): 5339. https://doi.org/10.3390/ijms26115339
Article Information
Publication history
Received: Jun 27, 2025
Accepted: Aug 20, 2025
Available online: Sep 3, 2025
Published: Sep 20, 2025
Copyright
© 2025 The Author(s); This is an open access article under the CC BY-NC license (https://creativecommons.org/licenses/by-nc/4.0/).
How to cite
Scherer, M. M., Hochecker, B., Matt, K. C., Meßmer, A. and Bergemann, J. (2025). Detection of Autophagy in Human Peripheral Blood Mononuclear Cells Using Guava® Autophagy and Flow Cytometry. Bio-protocol 15(18): e5457. DOI: 10.21769/BioProtoc.5457.
Category
Cell Biology > Cell-based analysis > Autophagic activity
Cell Biology > Cell-based analysis > Flow cytometry
Do you have any questions about this protocol?
Post your question to gather feedback from the community. We will also invite the authors of this article to respond.