- Protocols

- Articles and Issues
- For Authors
- About
- Become a Reviewer

Mouse Model of Lipopolysaccharide (LPS)-Induced Pulpitis
Published: Vol 15, Iss 2, Jan 20, 2025 DOI: 10.21769/BioProtoc.5128 Views: 3686
Reviewed by: Komuraiah MyakalaShivaram SelvamMinal EngavaleRaghavendra Yelahanka Nagaraja
Advertisement



Protocol Collections
Comprehensive collections of detailed, peer-reviewed protocols focusing on specific topics






Abstract
Pulpitis is an important and prevalent disease within the oral cavity. Thus, animal models are necessary tools for basic research focused on pulpitis. Researchers worldwide often use dogs and miniature pigs to construct animal models of pulpitis. However, gene editing in miniature pigs is difficult, the surgical modeling process is complex, and tooth demineralization time is lengthy. Although some researchers have attempted to establish a mouse model of pulpitis, most models have involved direct exposure of dental pulp. However, the causes of pulpitis vary considerably among individuals, hindering effective research. In this study, we established a mouse model of pulpitis by accessing the pulp cavity, exposing the pulp to lipopolysaccharide (LPS), and then filling the tooth. One day after surgery, we observed many necrotic tissues and extensive inflammatory exudate, including neutrophils, around the coronal cavity preparation. Additionally, we noted many more neutrophils and a small amount of chronic inflammatory cell infiltrates at the junction between inflamed and normal tissue. These findings indicated that our model can be used to explore the early stage of pulpitis. Ten days after surgery, we observed vacuolar degeneration in some fibroblasts and proliferation in others at the distal end of the inflamed tissue. We also noted dilation and congestion of the pulp blood vessels. Therefore, our model can also be used to explore the middle and later stages of pulpitis. Thirty days after surgery, we observed necrosis in the coronal pulp cavity and upper half of the root pulp, indicating that our model can also be used to explore the end stage of pulpitis. This model is easy to establish, shows pulpitis progression in the dental pulp, exhibits a clear inflammatory phenotype, and can be readily combined with gene editing techniques. Accordingly, it is suitable for basic research focused on pulpitis and has substantial practical value.
Key features
• Lipopolysaccharide (LPS) can induce pulpitis in mice.
• The mouse model of LPS-induced pulpitis can be used in basic studies of pulpitis.
• After 1 day, the mouse model of LPS-induced pulpitis can demonstrate the main phenotypes of early-stage pulpitis.
• After 10 days, the mouse model of LPS-induced pulpitis can display the main phenotypes of middle and late stage pulpitis.
Keywords: PulpitisGraphical overview
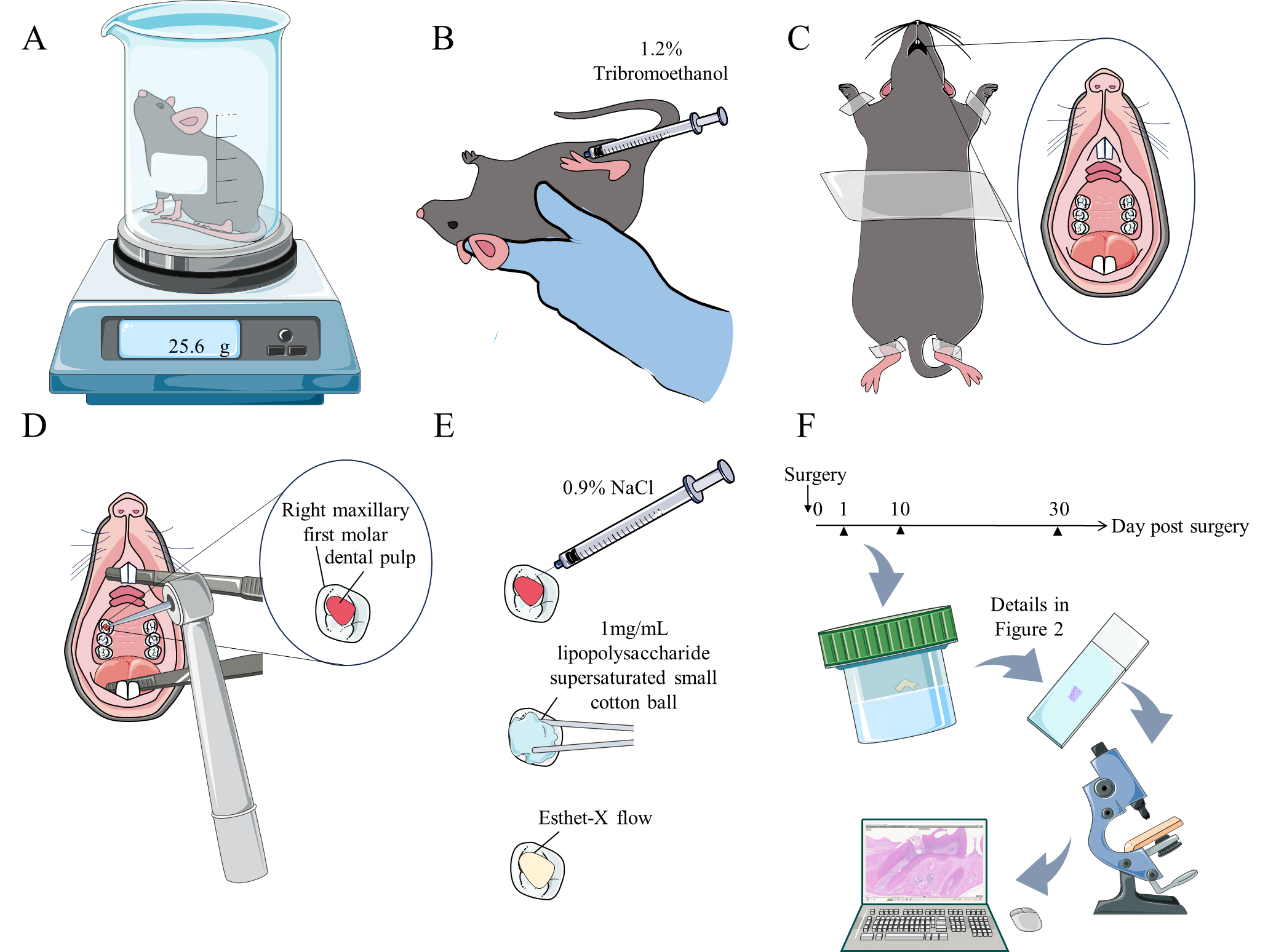
Figure 1. Graphical overview of the C57BL/6 mouse model of lipopolysaccharide (LPS)-induced pulpitis. A. Weigh the mouse. B. Anesthetize the mouse. C. Secure the mouse to the surgical pad and expose its oral cavity. D. Open the pulp chamber of the right maxillary first molar. E. Rinse the medullary foramen with 0.9% NaCl solution. Apply a small cotton ball saturated with 1 mg/mL LPS to the medullary foramen for 5 min, then cover the medullary foramen with Esthet-X flow and irradiate the site. F. Perform tissue decalcification and paraffin embedding (sample collection, decalcification, dehydration, wax embedding, and sectioning), followed by Histopathology staining, microscopy examination, image acquisition, and analysis.
Background
Although pulpitis is a common oral disease caused by anaerobic bacteria, its underlying mechanisms remain poorly understood. The construction of an animal model that simulates the processes involved in human pulpitis can aid in exploring the onset, progression, and outcomes of pulpitis. Thus far, pulpitis models have been constructed in animals such as mice, rats [1], ferrets, cats, dogs, miniature pigs, and monkeys [2]. However, because of their size, larger animals are more expensive and resource-intensive to maintain. Considering that experimental procedures in mice are relatively clear, gene editing is mainly conducted in these organisms, and the cost of mouse feed is low, there is a need to construct a mouse model of pulpitis.
Mouse molars are similar to human molars in many aspects, such as structure and cell types [3]; therefore, mouse models of pulpitis can be used to simulate the progression of human pulpitis. However, mouse molars are small, require skilled experimental techniques, and are difficult to manipulate; as such, mouse models of pulpitis have not been widely used. Most existing mouse models of pulpitis are induced by extended exposure of dental pulp after the pulp chamber has been opened [4–6]. This surgical method does not allow identification of the bacterial species causing pulpitis and is easily influenced by various biological factors, such as stimulant components in the feed and drink, or bacteria introduced into the oral cavity after surgery. In this study, we used lipopolysaccharide (LPS), an inflammatory factor often produced by anaerobic bacteria, as the pulpitis-inducing factor. After model induction, we capped the pulp to exclude interference from oral bacteria.
Materials and reagents
Biological materials
C57BL/6JCnc (B6J) mice (Beijing Vital River Laboratory Animal Technology Co., Ltd., Beijing)
Eight-week-old C57BL/6 mice, weighing 25–30 g, were purchased from Beijing Vital River Laboratory Animal Technology Co., Ltd. and maintained in a pathogen-free environment within Capital Medical University Animal Experiment Center. All animal experiments were approved by the ethics committee of Capital Medical University (AEEI-2024-071). Mice were maintained on a 12:12 h light/dark cycle and given food and water ad libitum. C57BL/6 mice, among the most popular inbred mouse strains in many research laboratories worldwide, were used in the experiments described below.
Reagents
LPS-Pg (InvivoGen, catalog number: tIrl-pglps)
Endotoxin-free water (InvivoGen, catalog number: h2olal-1.5)
Esthet-X flow (DENTSPLY DeTrey GmbH, catalog number: 005-SZ2648021)
75% ethyl alcohol (ANNJET, catalog number: Q/371402AAJ008)
Tribromoethanol (Sigma-Aldrich, catalog number: 75-80-9)
NaCl (Hong Kong JiSiEnBei International Trade Co., Ltd., catalog number: JS0492-1KG)
Tissue specimen fixative (Servicebio, catalog number: G1101-15ML)
Xylene (Sinopharm Group Chemical Reagent Co., Ltd., catalog number: 10023418)
Absolute ethanol (Sinopharm Group Chemical Reagent Co., Ltd., catalog number: 100092683)
Ethylenediaminetetraacetic acid (EDTA) decalcification solution (Servicebio, catalog number: G1105)
Benzyl alcohol (Sinopharm Group Chemical Reagent Co., Ltd., catalog number: 30020618)
Environmentally friendly dewaxing and clearing solution (Servicebio, catalog number: G1128-1L)
10% paraformaldehyde fixative (neutral) (Servicebio, catalog number: G1101)
H&E staining kit (Servicebio, catalog number: G1003)
Neutral gum (Sinopharm Group Chemical Reagent Co., Ltd., catalog number: 10004160)
Citric acid antigen repair solution (pH 6.0) (Servicebio, catalog number: G1202)
EDTA antigen repair solution (pH 9.0) (Servicebio, catalog number: G1203)
EDTA antigen repair solution (pH 8.0) (Servicebio, catalog number: G1206)
PBS buffer (Servicebio, catalog number: G0002)
Tissue autofluorescence quenching agent (Servicebio, catalog number: G1221)
Bovine serum albumin (BSA) (Servicebio, catalog number: GC305010)
DAPI staining reagent (Servicebio, catalog number: G1012)
Antifade mounting medium (Servicebio, catalog number: G1401)
MPO primary antibody (Servicebio, catalog number: GB15224)
DSPP primary antibody (Servicebio, catalog number: sc-73632)
Cy3-labeled goat anti-mouse IgG (Servicebio, catalog number: GB21301)
Goldner staining solution suit (Servicebio, catalog number: G1064)
Glacial acetic acid (Sinopharm Group Chemical Reagent Co., Ltd., catalog number: 10000218)
Hydrochloric acid (Sinopharm Group Chemical Reagent Co., Ltd., catalog number: 10011018)
Solutions
1.2% tribromoethanol (see Recipes)
0.9% NaCl (see Recipes)
1 mg/mL LPS-Pg (see Recipes)
95% ethyl alcohol (see Recipes)
90% ethyl alcohol (see Recipes)
85% ethyl alcohol (see Recipes)
1% hydrochloric acid alcohol solution (see Recipes)
0.2% glacial acetic acid (see Recipes)
Recipes
1.2% tribromoethanol
Reagent Final concentration Amount Tribromoethanol (absolute) 1.2% 0.12 g H2O n/a 10 mL Total n/a 10 mL Weigh 0.12 g of tribromoethanol using an electronic scale with 0.001 g accuracy and dissolve it in 10 mL of distilled water; then, mix thoroughly with a vortex mixer.
0.9% NaCl
Reagent Final concentration Amount NaCl (absolute) 0.9% 0.9 g H2O n/a 100 mL Total n/a 100 mL Weigh 0.9 g of NaCl using an electronic scale with 0.1 g accuracy and dissolve it completely in 100 mL of distilled water.
1 mg/mL LPS-Pg
Reagent Final concentration Amount LPS-Pg (absolute) 1 mg/mL 1 mg Endotoxin-free water n/a 1 mL Total n/a 1 mL Aspirate 1 mL of endotoxin-free water with a 1 mL injection syringe and inject it into a glass medicine bottle containing 1 mg of LPS-Pg powder; mix these components to obtain a 1 mg/mL LPS-Pg solution.
Aliquot and label the LPS-Pg solution in sterile 0.1 mL tubes and freeze them at -20 °C until use.
Note: LPS-Pg solution at a concentration of 100 mg/mL is stable for >6 months if stored at -20 °C.
95% ethyl alcohol
Reagent Final concentration Amount Absolute ethanol 95% 95 mL Distilled water n/a 5 mL Total n/a 100 mL Using a 100 mL graduated cylinder, measure 95 mL of absolute ethanol and transfer it to a 100 mL beaker. Using a 5 mL graduated cylinder, measure 5 mL of distilled water and add it to the beaker containing ethanol. Add a magnetic stir bar to the beaker, place the beaker on a magnetic stirrer, and stir for 5 min.
90% ethyl alcohol
Reagent Final concentration Amount Absolute ethanol 90% 90 mL Distilled water n/a 10 mL Total n/a 100 mL Using a 100 mL graduated cylinder, measure 90 mL of absolute ethanol and transfer it to a 100 mL beaker. Using a 10 mL graduated cylinder, measure 10 mL of distilled water and add it to the beaker containing ethanol. Add a magnetic stir bar to the beaker, place the beaker on a magnetic stirrer, and stir for 5 min.
85% ethyl alcohol
Reagent Final concentration Amount Absolute ethanol 85% 85 mL Distilled water n/a 15 mL Total n/a 100 mL Using a 100 mL graduated cylinder, measure 85 mL of absolute ethanol and transfer it to a 100 mL beaker. Using a 25 mL graduated cylinder, measure 15 mL of distilled water and add it to the beaker containing ethanol. Add a magnetic stir bar to the beaker, place the beaker on a magnetic stirrer, and stir for 5 min.
1% hydrochloric acid alcohol solution
Reagent Final concentration Amount Hydrochloric acid 1% 1,000 μL Absolute alcohol n/a 99 mL Total n/a 100 mL Using a 100 mL graduated cylinder, measure 99 mL of absolute ethanol and transfer it to a 100 mL beaker. Using a 1,000 μL pipette, measure 1,000 μL of hydrochloric acid and add it to the beaker containing ethanol. Add a magnetic stir bar to the beaker, place the beaker on a magnetic stirrer, and stir for 30 s.
0.2% glacial acetic acid
Reagent Final concentration Amount Glacial acetic acid 0.2% 200 μL Distilled water n/a 99.8 mL Total n/a 100 mL Using a 200 μL pipette, measure 200 μL of glacial acetic acid and add it to a 100 mL volumetric flask. Add distilled water to the flask while stirring with a glass rod until the solution reaches a volume of 100 mL.
Laboratory supplies
Diamond bur (MANI, catalog number: TC-SS21F)
Dental file (Velbon, catalog number: K23120)
Operating scissors (Velbon, catalog number: J21030)
Ophthalmic forceps, straight (Velbon, catalog number: JD1050)
Ophthalmic forceps, curved (Velbon, catalog number: JD1060)
Dressing forceps (Velbon, catalog number: J42035)
Icebox (Biosharp, catalog number: BC032)
Icebox, silicone base (Biosharp, catalog number: BC034)
1 mL injection syringe (needle dimensions: 0.45 × 15 mm)
Pipette (10 μL, 200 μL, 1,000 μL) (Servicebio, catalog numbers: SPIP-10, SPIP-200, SPIP-1000)
Bagged tips (10 μL, 200 μL, 1,000 μL) (Servicebio, catalog numbers: P-10, P-200, P-1000)
0.1 mL centrifuge tubes (Thermo Fisher Scientific, catalog number: 4358297)
0.1 mL centrifuge tube rack (Servicebio, catalog number: WGH002)
Nitrile gloves (Servicebio, catalog number: GN1801M)
Stainless-steel lunch box (China Industry Union, catalog number: WGH0001)
Oral surgery kit (HENAN SHENG YUBEI EISAI Co., Ltd., catalog number: 20202171244)
Medical adhesive tape
Medical cotton balls: large and small
Permanent ink markers
Square medical sharps container
Medical waste garbage bags
Beaker
Doctor's scrubs
Embedding frame (Servicebio, catalog number: EF-1)
Ophthalmic scissors (Velbon, catalog number: JC2303)
Immunohistochemical pen (Servicebio, catalog number: G6100)
Graduated cylinder (5 mL, 10 mL, 25 mL, 100 mL)
Magnetic stirrer (Servicebio, catalog number: MS-150)
Magnetic stir bar (Servicebio, catalog number: WGA0023)
Volumetric flask (100 mL)
Equipment
Electronic scale with 0.1 g accuracy (LICHEN, catalog number: YP10001B)
Electronic scale with 0.001 g accuracy (Sartorius, catalog number: BCA224I-1OCN)
-20 °C freezer (MeiLing, catalog number: DW-YL450)
Autoclave (China Industry Union)
Head-mounted dental loupe (3.5×, black, 5 W headlight, China Industry Union)
Vortex mixer (Servicebio, catalog number: SMV-3500)
Portable dental treatment machine (Greeloy, catalog number: GU-P206S)
Timer
Dehydrator (DIAPATH, model: Donatello)
Embedding machine (Wuhan Junjie Electronics Co., Ltd., catalog number: JB-P5)
Freezing platform (Wuhan Junjie Electronics Co., Ltd., catalog number: JB-L5)
Constant temperature shaker (TIANJIN LEIBO TERRY EQUIPMENT Co., Ltd., catalog number: ZHPW-250)
Microtome (Shanghai Leica Instrument Co., Ltd., catalog number: RM2016)
Tissue spreader (Zhejiang Kehua Instrument Co., Ltd., catalog number: KD-P)
Oven (Tianjin Laibo Rui Instrument Equipment Co., Ltd., catalog number: GFL-230)
Adhesive slides (Servicebio, catalog number: G6012)
Cover glass (Citotest Labware Manufacturing Co., Ltd., catalog number: 10212432C)
Upright optical microscope (Nikon, model: NIKON ECLIPSE E100)
Imaging system (Nikon, model: NIKON DS-U3)
Decolorization shaker (Servicebio, catalog number: DS-2S100)
Microwave oven (Galanz, catalog number: P70D20TL-P4)
Scanner (3DHISTECH, model: Pannoramic MIDI)
Software and datasets
CaseViewer (Version: 2.4; Copyright © 2001-2020 3DHISTECH Ltd.; Build: 2.4.0.119028)
ImageJ 1.54f (Wayne Rasband and contributors; National Institutes of Health, USA)
Procedure
Preparation
Prepare Recipes 1–8 following the instructions provided in Recipes section.
Autoclaving of the modeling instruments: Within 1–5 days before modeling, place the modeling instruments in a stainless-steel lunch box and sterilize them using an autoclave.
Modeling surgery
Anesthesia
Weigh the C57BL/6 mouse using a beaker and an electronic scale with 0.1 g accuracy. Use 1.2% tribromoethanol (see Recipes) for anesthesia (intraperitoneal injection), with a dosage of 0.5 mL per 20 g body weight (Figure 1A, B).
Fixing
Pinch the mouse’s toe to check its reaction. If the mouse does not respond when its toe is pinched, the mouse has reached a deep level of anesthesia. Then, secure the mouse to the surgical pad with medical adhesive tape; this will ensure that the mouse cannot interrupt the surgery (Figure 1C).
Opening the pulp chamber
Open the mouse’s oral cavity with curved ophthalmic forceps. Use dressing forceps to expand the oral cavity and protect the tongue, thus preventing injury by the diamond bur; concurrently, completely expose the upper portion of the mouth.
Use the diamond bur to access the maxillary first molar in the mouse, then expand the pulp exposure with the dental file; the final diameter of exposure should be approximately 1 mm. From the exposure, white and slightly red dental pulp tissue should be visible (Figure 1D).
Rinsing
Aspirate 0.1 mL of 0.9% NaCl solution (see Recipes) with a 1 mL injection syringe. Place the tip of the needle over the medullary foramen and quickly empty the syringe to flush out any dentin debris that may have entered the medullary foramen.
LPS induction
Extract 10 μL of 1 mg/mL LPS-Pg (see Recipes) into a 0.1 mL centrifuge tube. Use straight ophthalmic forceps to completely saturate a small cotton ball in the LPS-Pg solution. Keep the saturated small cotton ball on the exposed pulp for 5 min.
Pulp capping and tooth filling
Remove the cotton ball and restore the tooth with Esthet-X flow (Figure 1E).
After surgery, loosen the mouse’s restraints; return the mouse to the cage after it has awakened.
Real surgical images can be found in Figure S1.
Tissue decalcification and paraffin embedding (Figure 2C)
Sample collection
After day 1 and 10 of model establishment, sacrifice the mouse by cervical dislocation; carefully harvest maxillary tissue with straight ophthalmic forceps tweezers and ophthalmic scissors. Place the maxillary tissues into a 15 mL centrifuge tube with 10% paraformaldehyde fixative (neutral) and incubate at room temperature for 24 h.
Decalcification
Place printed labels and tissues in sequential order in an embedding frame. Then, place them in a basin, fill it with fresh decalcification solution, seal the container, and store all components in a constant temperature shaker at 25 °C with a speed of 110 RPM. This process results in decalcification. The decalcification solution should be replaced every 2–3 days. The degree of decalcification should be observed by pricking the tissue with a needle every 2 days. If the needle can be moved in the tissue, cut a plane with a Lycra blade along the edge of the maxillary tissue to remove excess tissue and ensure that the embedding surface is flat, which can accelerate the softening speed.

Figure 2. Operation process of tissue decalcification and paraffin embedding, HE staining, immunofluorescent staining, and immunofluorescent stainingDehydration and wax infiltration
Remove the softened tissue from the decalcification solution, rinse with tap water for 5 h, place it into a dehydrating basket, and dehydrate using an alcohol gradient in the dehydrator. Prepare reagents for dehydration and wax infiltration: alcohol (75%, 85%, 90%, 95%), anhydrous ethanol (divide the liquid into three separate bottles labeled I, II, and III), benzyl alcohol, xylene (divide the liquid into two separate bottles labeled I and II), and melted paraffin (divide the liquid into three separate bottles labeled I, II, and III). The dehydration and wax infiltration steps are as follows: 75% alcohol for 2 h, 85% alcohol for 2 h, 90% alcohol for 1.5 h, 95% alcohol for 2 h, anhydrous ethanol I for 2 h, anhydrous ethanol II for 2 h, benzyl alcohol for 40 min, xylene I for 40 min, xylene II for 40 min, melted paraffin I for 0.5 h at 65 °C, melted paraffin II for 1 h at 65 °C, and melted paraffin III for 2 h 45 min at 65 °C.
Embedding
Transfer the wax-infiltrated tissue to the embedding machine. First, place the melted wax into the embedding frame. Then, place the tissue into the embedding frame according to the requirements of the embedding surface, and attach appropriate labels before the wax solidifies. Cool the wax on a -20 °C freezing platform. After solidification, remove the wax block from the embedding frame and trim it.
Sectioning
Use the trimmed wax block to prepare 4 μm thick paraffin sections. Float sections in warm water at 40 °C to flatten the tissue. Collect the sections and bake them in an oven at 60 °C. After the water has evaporated and the wax has melted, store the sections at room temperature.
HE staining (Figure 2D)
Dewaxing and rehydration
Prepare reagents: environmentally friendly dewaxing and clearing solution (divide the liquid into two separate bottles labeled I and II), anhydrous ethanol (divide the liquid into two separate bottles labeled I and II), and 75% ethyl alcohol. Immerse paraffin sections in the following sequence: environmentally friendly dewaxing and clearing solution I for 20 min, environmentally friendly dewaxing and clearing solution II for 20 min, anhydrous ethanol I for 5 min, anhydrous ethanol II for 5 min, and 75% ethyl alcohol for 5 min. Subsequently, rinse with tap water.
Hematoxylin staining
Stain the sections with hematoxylin solution for 3–5 min and rinse with tap water. Next, immerse the sections in hematoxylin differentiation solution and rinse with tap water. Finally, immerse the sections in hematoxylin bluing solution and rinse with tap water.
Eosin staining
Immerse sections in the following sequence of solutions: 85% ethanol for 5 min, 95% ethanol for 5 min, and eosin dye for 5 min.
Dehydration and sealing
Prepare reagents for dehydration and wax infiltration: absolute ethanol (divide the liquid into three separate bottles labeled I, II, and III) and xylene (divide the liquid into two separate bottles labeled I and II). Immerse sections in the following sequence of solutions: absolute ethanol I for 5 min, absolute ethanol II for 5 min, absolute ethanol III for 5 min, xylene for 5 min, and xylene for 5 min. Then, seal the sections with neutral gum.
Immunofluorescence staining (Figure 2E)
Dewaxing and rehydration
Prepare reagents: environmentally friendly dewaxing and clearing solution (divide the liquid into three separate bottles labeled I, II, and III) and anhydrous ethanol (divide the liquid into three separate bottles labeled I, II, and III). Sequentially immerse the sections in the following sequence: environmentally friendly dewaxing and clearing solution I for 10 min, environmentally friendly dewaxing and clearing solution II for 10 min, environmentally friendly dewaxing and clearing solution III for 10 min, absolute ethanol I for 5 min, absolute ethanol II for 5 min, and absolute ethanol III for 5 min. Subsequently, rinse with tap water.
Antigen retrieval
Place the sections in a water bath for 30 min. After retrieval is complete, allow sections to cool naturally. Wash the sections three times in PBS (pH 7.4) on a decolorization shaker for 5 min per wash.
Serum blocking
Dry the sections and use a hydrophobic pen to draw a circle around the tissue. Apply 3% BSA for 30 min to block nonspecific binding.
Primary antibody incubation
Prepare primary antibody: dilute the primary antibodies (DSPP 1:100; MPO 1:500) in PBS buffer. Add the diluted primary antibody to the sections, ensuring that they are lying flat in a humidified chamber. Incubate overnight at 4 °C.
Secondary antibody incubation
Wash the sections three times in PBS (pH 7.4) on a decolorization shaker for 5 min per wash. Add the secondary antibody (Cy3-labeled goat anti-mouse IgG) and incubate for 50 min at room temperature in the dark.
Stain cell nuclei with DAPI
Wash the sections three times in PBS (pH 7.4) on a decolorization shaker for 5 min per wash. Add the DAPI staining reagent and incubate for 10 min at room temperature in the dark.
Quench tissue autofluorescence and sealing
Wash the sections three times in PBS (pH 7.4) on a decolorization shaker for 5 min per wash. Add tissue autofluorescence quenching agent B and incubate for 10 min at room temperature in the dark. Use antifade mounting medium to seal the sections.
Goldner trichrome staining (Figure 2F)
Dewaxing and rehydration
Prepare reagents: Xylene (divide the liquid into two separate bottles labeled I and II), anhydrous ethanol (divide the liquid into two separate bottles labeled I and II), and 75% ethyl alcohol. Sequentially immerse the paraffin sections in the following sequence: xylene I for 20 min, xylene II for 20 min, anhydrous ethanol I for 5 min, anhydrous ethanol II for 5 min, and 75% ethyl alcohol for 5 min. Subsequently, rinse with tap water.
Nuclear staining
Mix Goldner staining solution A and Goldner staining solution B in equal proportions. Place sections in the mixed solution and stain for 20 min. Wash with tap water, then differentiate with 1% hydrochloric acid alcohol solution for 2 s. Rinse with tap water, then wash with distilled water.
Staining with Goldner staining solution C
Immerse sections in the first jar of Goldner staining solution C for 10 min, then quickly rinse with 0.2% glacial acetic acid (3 s per rinse).
Staining with Goldner staining solution D
Immerse sections in Goldner staining solution D for 3 min. Monitor the staining under a microscope; ensure that Goldner staining solution C fades from the collagen areas.
Staining with Goldner staining solution C
Immerse sections in the second jar of Goldner staining solution C for 5 min, then quickly rinse with 0.2% glacial acetic acid (3 s per rinse).
Staining with Goldner staining solution E
Immerse sections in Goldner staining solution E for 5 min. Then, differentiate the stain using three jars of 0.2% glacial acetic acid (2 s per jar). Dehydrate the sections using three jars of anhydrous ethanol (2 s, 3 s, and 5 s, respectively).
Clearing and sealing
Place sections in the third jar of anhydrous ethanol for 5 min. Clear the sections in xylene for 5 min. Finally, seal with neutral gum.
Perform microscopy examination, image acquisition, and analysis (Figure 1F)
HE staining: Nuclei will be stained blue, whereas cytoplasm will be stained red.
Immunofluorescence staining: DAPI (excitation wavelength 330–380 nm, emission wavelength 420 nm) will stain nuclei blue, whereas Cy3 (excitation wavelength 510–560 nm, mission wavelength 590 nm) will stain the target protein red.
Goldner trichrome staining: mineralized bone will be stained green, whereas non-mineralized tissue will be stained orange red.
Data analysis
HE staining results
Following above procedures (A–D, G), we constructed a mouse model of LPS-induced pulpitis (LPS surgery mice). To verify that pulpitis was induced by LPS, we established a solvent control group in which 1 mg/mL LPS was replaced with an equal volume of endotoxin-free water, and the same procedure was followed (solvent surgery mice).
We analyzed the HE staining results of LPS surgery mice and solvent surgery mouse models of pulpitis at 1 day (1 d), 10 d, and 30 d after surgery using Case Viewer and ImageJ. In the early stage of pulpitis, the primary manifestation is exudation. At 1 d post-surgery in LPS surgery mice (Figure 3A-A2), we observed a large number of necrotic tissues and extensive inflammatory exudate, including neutrophils, around the coronal cavity preparation (black arrow). Additionally, we noted many more neutrophils and a small amount of chronic inflammatory cell infiltrates at the junction between inflamed and normal tissue (black ellipse). These findings indicate that our model can be used to explore the early stages of pulpitis. After the early stage, pulpitis gradually transitions from exudation to hyperplasia, denoting the middle and later stages. In the middle and later stages, the primary manifestation is hyperplasia; this mainly includes fibroblast proliferation, blood vessel dilation, and the proliferation of chronic inflammatory cells. At 10 d post-surgery in LPS surgery mice (Figure 3B-B2), we observed vacuolar degeneration in some fibroblasts (blue arrow) and proliferation in others at the distal end of inflamed tissue (blue ellipse). Additionally, the pulp blood vessels were dilated and congested (black triangle). These observations suggest that our model can also be used to explore the middle and later stages of pulpitis. In the end stage, the final outcome typically comprises necrosis, although recovery is possible. At 30 d post-surgery in LPS surgery mice (Figure 3C-C2), we observed inflammation invading the coronal pulp cavity and most of the root pulp. The coronal pulp cavity and upper half of the root pulp were necrotic. Furthermore, necrotic tissue and inflammatory exudate, including neutrophils, were present around the coronal cavity preparation and right root canal (black arrow). These findings indicate that our model can be used to explore the end stage of pulpitis. Analysis with ImageJ revealed that the proportion of inflamed areas gradually increased with prolonged inflammation (Figure 3G). These results revealed obvious symptoms of pulpitis, confirming the successful establishment of our model.
The solvent control group did not exhibit a favorable inflammatory phenotype (Figure 3D–F). Comparisons of A with D, B with E, and C with F in Figure 3 indicate that LPS is necessary for the successful induction of pulpitis.
To investigate whether 1 mg/mL LPS is the optimal concentration for pulpitis induction, we established high-concentration (10 mg/mL) and low-concentration (0.1 mg/mL) groups, then followed the same procedure (Figure S2). The experimental results showed that pulpitis induced by 0.1 mg/mL LPS was too mild and obvious pulp repair could be seen, which could not reflect the development process of pulpitis. However, the inflammation induced by 10 mg/mL LPS was too heavy, and tissue disintegration occurred on the first day; pulpitis progressed too fast, it was not easy to observe the complete inflammatory process, the consumption of LPS reagent was large, and the cost was higher. In summary, the pulpitis model constructed with 1 mg/mL LPS exhibited the most complete pulpitis progression and was the most suitable concentration for constructing this model.
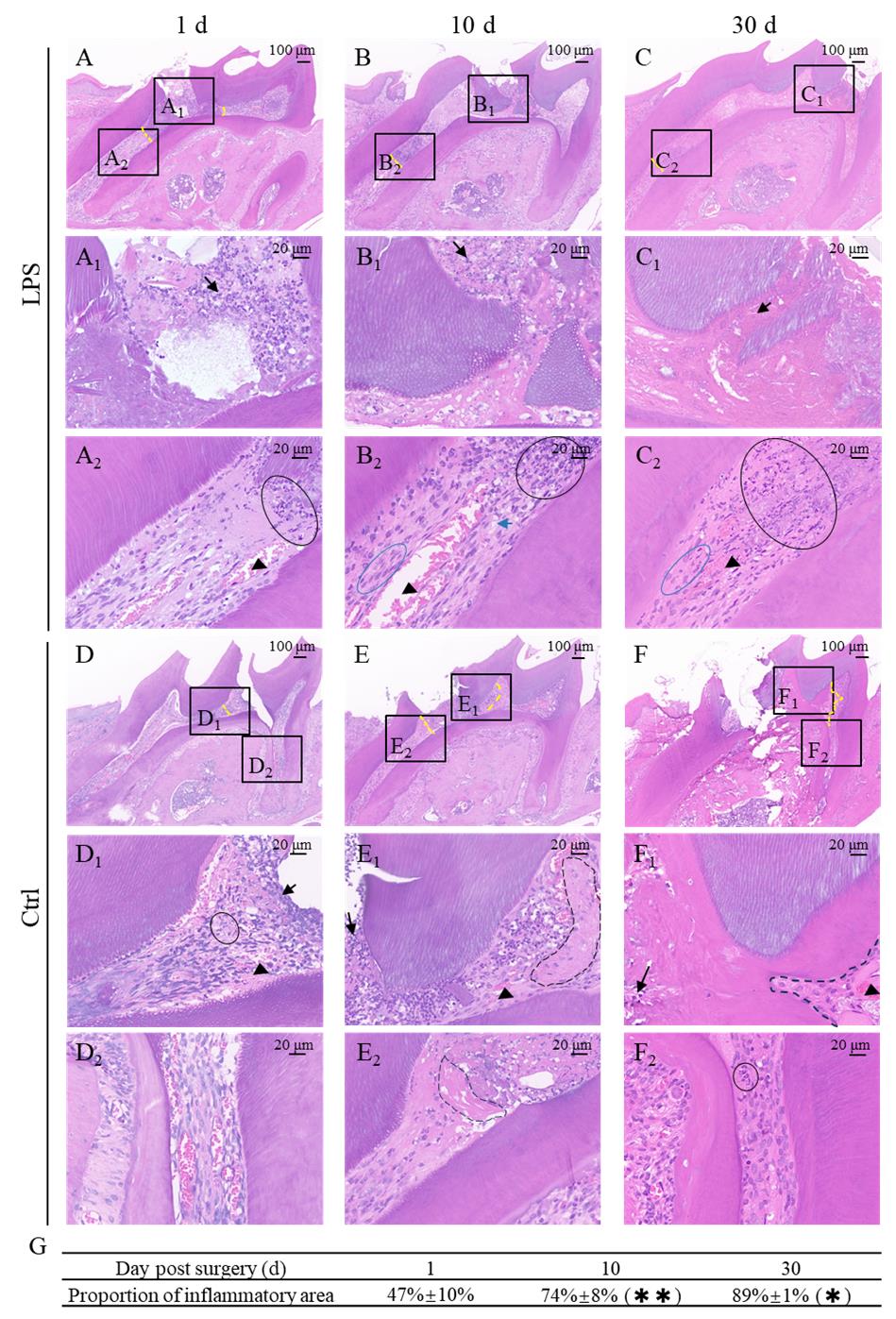
Figure 3. HE staining results for lipopolysaccharide (LPS) surgery mouse and solvent surgery mouse (1, 10, and 30 days post-surgery). A. 1 d post-surgery in LPS surgery mouse: Inflammation has not invaded the root pulp. A1: A large number of necrotic tissues and extensive inflammatory exudate, including neutrophils, are present around the coronal cavity preparation (black arrow). Many more neutrophils and a small amount of chronic inflammatory cell infiltrates are evident at the junction between inflamed and normal tissue (black ellipse). The pulp blood vessels are dilated and congested (black triangle). A2: The root pulp appears normal. B. 10 d post-surgery in LPS surgery mouse: Inflammation has invaded the coronal pulp cavity and upper portion of root pulp. B1: A large number of necrotic tissues and extensive inflammatory exudate, including neutrophils, are present around the coronal cavity preparation (black arrow). Many disintegrated neutrophils and substantial chronic inflammatory cell infiltrates are evident at the junction between inflamed and normal tissue (black ellipse). B2: Fibroblasts exhibit vacuolar degeneration (blue arrow) and proliferate at the distal end of inflamed tissue (blue ellipse). The pulp blood vessels are dilated and congested (black triangle). Necrotic tissue is visible in the upper portion of root pulp, whereas the lower portion of root pulp appears normal. C. 30 d post-surgery in LPS surgery mouse: Inflammation has invaded the coronal pulp cavity and most of the root pulp. The coronal pulp cavity and upper half of the root pulp are necrotic. C1: Necrotic tissue and inflammatory exudate, including neutrophils, are present around the coronal cavity preparation and right root canal (black arrow). C2: Many disintegrated neutrophils and substantial chronic inflammatory cell infiltrates are evident at the junction between inflamed and normal tissue (black ellipse). Fibroblasts are proliferating beneath the necrotic tissue (blue ellipse). The pulp blood vessels are dilated and congested (black triangle). D. 1 d post-surgery in solvent surgery mouse: Inflammation has not invaded the root pulp. D1: A small amount of inflammatory exudate is evident around the coronal cavity preparation (black arrow); intratissue hemorrhage is present, and pulp blood vessels under the inflammatory exudate are congested (black triangle). Some neutrophils and chronic inflammatory cell infiltrates can be observed (black ellipse). D2: The root pulp appears normal. E. 10 d post-surgery in solvent surgery mouse: Inflammation has invaded a small portion of the root pulp. E1: A large amount of inflammatory exudate, including neutrophils, is visible around the coronal cavity preparation (black arrow). Fibroblasts are secreting collagen fiber bundles to contain the inflammation (broken line). The pulp blood vessels are congested (black triangle). E2: Pre-mineralized tissue is present beneath the inflammatory exudate (broken line). The root pulp appears normal. F. 30 d post-surgery in solvent surgery mouse: Inflammation has invaded the root pulp. F1: A small amount of inflammatory exudate including neutrophils and chronic inflammatory cells are observed around coronal cavity preparation (black arrow). Fibrous matrix proliferates and fills part of the pulp cavity (broken line). The pulp blood vessels are congested (black triangle). F2: Some neutrophils and chronic inflammatory cell infiltrates are present in the root pulp (black ellipse). G. Analysis of the proportion of inflamed area at 1 d, 10 d, and 30 d post-surgery in LPS surgery mice (47% ± 10%, 74% ± 8%, and 89% ± 1%, respectively). The proportion of inflamed areas at 10 d post-surgery in LPS surgery mice significantly increased compared with 1 d post-surgery in LPS surgery mice (P < 0.01). The proportion of inflamed areas at 30 d post-surgery in LPS surgery mice significantly increased compared with 10 d post-surgery in LPS surgery mice (P < 0.05).Immunofluorescence staining results
With the LPS-induced pulpitis model sections obtained in procedure C, we performed subsequent immunofluorescence staining (procedure E) with MPO as the staining indicator. Myeloperoxidase (MPO), also known as peroxidase, is derived from neutrophils, monocytes, and macrophages. In the process of inflammation, white blood cells release a large amount of MPO, so the detection of MPO expression can reflect the severity of inflammation. In Figure 4A, DAPI channel nuclei are shown in blue and MPO is shown in red. It could be observed that with the extension of LPS modeling time, the proportion of MPO positive areas increased significantly (P < 0.001, Figure 4B), indicating that the inflammation was gradually aggravated, suggesting that the modeling was successful.
Goldner trichrome staining results
With sections of LPS-induced pulpitis model obtained in procedure C, we performed subsequent Goldner trichrome staining (procedure F). Goldner trichrome staining can distinguish between mineralized bone (green) and non-mineralized tissue (orange red). In Figure 5, it can be seen that with the extension of modeling time, more and more mineralized tissues in the dental pulp of mice tended to form mature mineralized tissues, which successfully demonstrated the progress of pulpitis and proved the success of modeling.
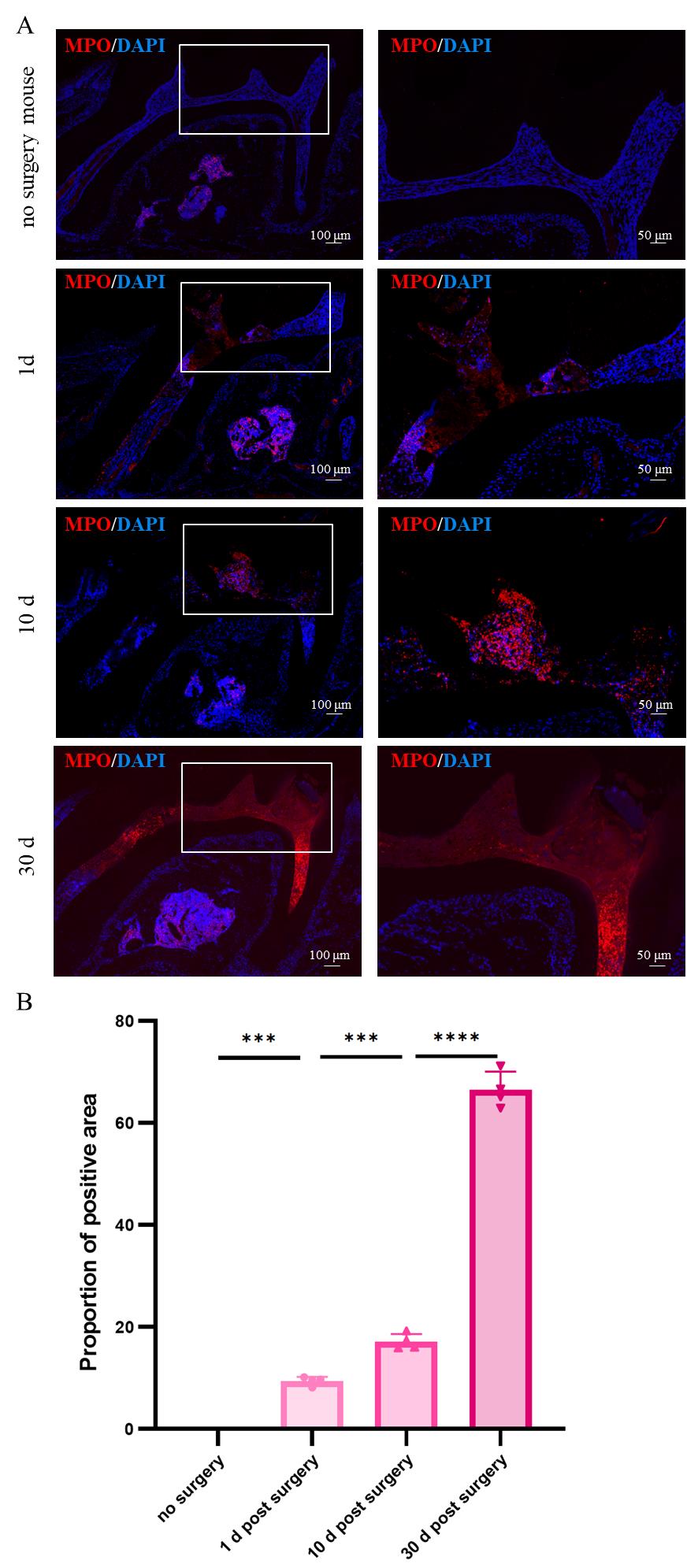
Figure 4. Immunofluorescence staining results for no-surgery mouse and lipopolysaccharide (LPS) surgery mouse (1, 10, and 30 days post-surgery). A. Immunofluorescence staining results; red represents MPO and blue represents DAPI. B. Analyzing the proportion of positive areas in no-surgery, 1 d, 10 d, and 30 d post-surgery mice. MPO, myeloperoxidase.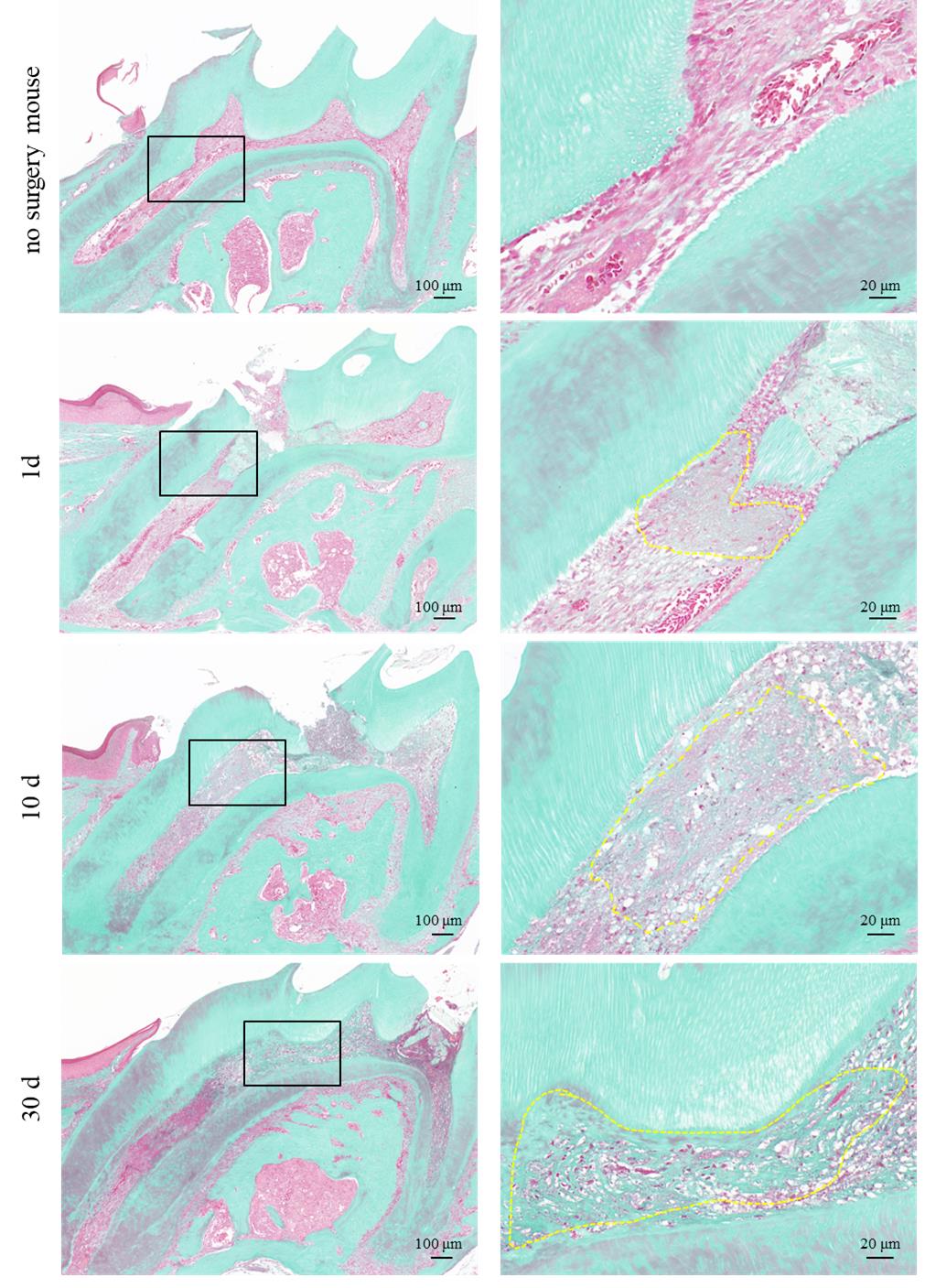
Figure 5. Goldner trichrome staining results for no-surgery mouse and lipopolysaccharide (LPS) surgery mouse (1, 10, and 30 days post-surgery). No-surgery mouse shows no green in pulp cavity. 1 d post-surgery mouse shows punctate light green. 10 d post-surgery mouse shows thin cord-like and meshy light green in the coronal pulp. 30 d post-surgery mouse shows dense green in the coronal pulp diffusely and cord-like light green in distal pulp.
Validation of protocol
All four mice had induced pulpitis by LPS (Figure 3, 4, and 5), which sufficiently validated this protocol.
General notes and troubleshooting
Because the mouse’s oral cavity is small and it is difficult to obtain an appropriate mouth-opening device, we used dressing forceps to open the mouths of mice in this study. However, to prevent mandibular dislocation and adverse effects (e.g., incomplete mouth closure) related to the extended use of dressing forceps for mouth opening, straight ophthalmic forceps can be used for mouth opening after pulp exposure; this approach reduces damage to the maxillary and mandibular joints.
During the feeding period after modeling, the Esthet-X flow used to close the opening hole can fall off due to nibbling feed or bedding, which will lead to modeling failure. In order to avoid this situation, we use shavings cushion material and soft pasty feed after modeling. This operation can effectively avoid the shedding of Esthet-X flow.
Acknowledgments
This work was supported by the China National Natural Science Foundation (82071074); 2023-PUMCH-E-010.
Competing interests
The authors declare no competing interests.
Ethical considerations
All animal experiments were approved by the ethics committee of Capital Medical University (AEEI-2024-071).
References
- Huang, H., Okamoto, M., Watanabe, M., Matsumoto, S., Moriyama, K., Komichi, S., Ali, M., Matayoshi, S., Nomura, R., Nakano, K., et al. (2023). Development of Rat Caries-Induced Pulpitis Model for Vital Pulp Therapy. J Dent Res. 102(5): 574–582.
- Aubeux, D., Renard, E., Pérez, F., Tessier, S., Geoffroy, V. and Gaudin, A. (2021). Review of Animal Models to Study Pulp Inflammation. Front Dent Med. 2: e673552.
- Krivanek, J., Soldatov, R. A., Kastriti, M. E., Chontorotzea, T., Herdina, A. N., Petersen, J., Szarowska, B., Landova, M., Matejova, V. K., Holla, L. I., et al. (2020). Dental cell type atlas reveals stem and differentiated cell types in mouse and human teeth. Nat Commun. 11(1): 4816.
- Shi, X., Li, Z., He, Y., Jiang, Q. and Yang, X. (2017). Effect of different dental burs for experimental induction of pulpitis in mice. Arch Oral Biol. 83: 252–257.
- He, Y., Gan, Y., Lu, J., Feng, Q., Wang, H., Guan, H. and Jiang, Q. (2017). Pulpal Tissue Inflammatory Reactions after Experimental Pulpal Exposure in Mice. J Endod. 43(1): 90–95.
- Erdogan, O., Xia, J., Chiu, I. M. and Gibbs, J. L. (2023). Dynamics of Innate Immune Response in Bacteria-Induced Mouse Model of Pulpitis. J Endod. 49(11): 1529–1536.
- Chung, M. K., Lee, J., Duraes, G. and Ro, J. (2011). Lipopolysaccharide-induced Pulpitis Up-regulates TRPV1 in Trigeminal Ganglia. J Dent Res. 90(9): 1103–1107.
Supplementary information
The following supporting information can be downloaded here:
- Figure S1. Images of the surgical procedure
- Figure S2. HE staining results for 0.1 mg/mL, 1 mg/mL, 10 mg/mL LPS surgery mouse (1 d and 10 d post-surgery) and no surgery mouse
Article Information
Publication history
Received: Apr 1, 2024
Accepted: Oct 5, 2024
Available online: Oct 23, 2024
Published: Jan 20, 2025
Copyright
© 2025 The Author(s); This is an open access article under the CC BY-NC license (https://creativecommons.org/licenses/by-nc/4.0/).
How to cite
Shao, L., Chen, B. and Zheng, Y. (2025). Mouse Model of Lipopolysaccharide (LPS)-Induced Pulpitis. Bio-protocol 15(2): e5128. DOI: 10.21769/BioProtoc.5128.
Category
Biological Sciences > Biological techniques
Medicine > Inflammation
Do you have any questions about this protocol?
Post your question to gather feedback from the community. We will also invite the authors of this article to respond.