

Transient Middle Cerebral Artery Occlusion with an Intraluminal Suture Enables Reproducible Induction of Ischemic Stroke in Mice
经腔内缝合的短暂性大脑中动脉闭塞可重复诱导小鼠缺血性脑卒中
(*contributed equally to this work) 发布: 2022年02月05日第12卷第3期 DOI: 10.21769/BioProtoc.4305 浏览次数: 8232
评审: Nafisa M. JadavjiMaria NguyenAnonymous reviewer(s)

参见作者原研究论文
The authors used this protocol in:
Mar 2021
Advertisement











Abstract
Ischemic stroke is a leading cause of mortality and chronic disability worldwide, underscoring the need for reliable and accurate animal models to study this disease’s pathology, molecular mechanisms of injury, and treatment approaches. As most clinical strokes occur in regions supplied by the middle cerebral artery (MCA), several experimental models have been developed to simulate an MCA occlusion (MCAO), including transcranial MCAO, micro- or macro-sphere embolism, thromboembolisation, photothrombosis, Endothelin-1 injection, and – the most common method for ischemic stroke induction in murine models – intraluminal MCAO. In the intraluminal MCAO model, the external carotid artery (ECA) is permanently ligated, after which a partially-coated monofilament is inserted and advanced proximally to the common carotid artery (CCA) bifurcation, before being introduced into the internal carotid artery (ICA). The coated tip of the monofilament is then advanced to the origin of the MCA and secured for the duration of occlusion. With respect to other MCAO models, this model offers enhanced reproducibility regarding infarct volume and cognitive/functional deficits, and does not require a craniotomy. Here, we provide a detailed protocol for the surgical induction of unilateral transient ischemic stroke in mice, using the intraluminal MCAO model.
Graphic abstract:

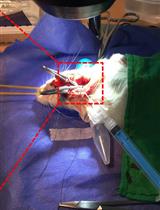
Overview of the intraluminal monofilament method for transient middle cerebral artery occlusion (MCAO) in mouse.
Background
With a global prevalence of more than 101.5 million, stroke is a leading cause of mortality and chronic disability worldwide (Benjamin et al., 2019; Diseases and Injuries, 2020). Though some strokes are caused when a vessel ruptures (i.e., hemorrhagic stroke), ischemic strokes account for 87% of clinical cases and occur following vascular occlusion, either by local arterial thrombus formation (e.g., cerebral atherosclerotic stroke) or a traveling embolic clot (e.g., cardioembolism) (Virani et al., 2021). Acute interventions to restore perfusion and halt neuronal death include pharmacological thrombolysis [i.e., intravenous recombinant tissue plasminogen activator (rtPA)] and mechanical endovascular thrombectomy (Pierot et al., 2018; Powers et al., 2018; Adams and Nudo, 2013), though clinical exclusion criteria restrict eligibility to just 20% of patients (National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group, 1995; Hacke et al., 2008; Saver et al., 2009; Smith and Furlan, 2016; Yaghi et al., 2017; Evans et al., 2017; Albers et al., 2018; Nogueira et al., 2018; Powers et al., 2018; Mokin et al., 2018).
The necessity for more inclusive therapeutic options underscores the significance of animal models, which have long been used to study disease pathology, identify molecular mechanisms of injury, and test treatment paradigms (Narayan et al., 2021). While large animal models (i.e., pigs, dogs, non-human primates) serve a key role, given their higher order resemblance to the human condition (Kaiser and West, 2020), small animals are most commonly used in preclinical stroke research. Factors specifically favoring murine models (i.e., mice and rats) include lower cost, reliable physiological responses, procedural reproducibility, available imaging modalities, a variety of functional and behavioral tests, and options for genetic manipulation (Fluri et al., 2015; Hermann et al., 2019).
The majority of clinical strokes occur in regions supplied by the middle cerebral artery (MCA), a terminal branch of the internal carotid artery (ICA) that supplies two-thirds of the lateral cortex, the infra-lateral surface of the anterior brain, and many deep subcortical structures (e.g., internal capsule and basal ganglia) (Nogles and Galuska, 2021). Numerous preclinical approaches to experimental MCA occlusion (MCAO) have been described, including direct suturing or electrocoagulation of the MCA (transcranial MCAO), intraluminal placement of a monofilament (intraluminal MCAO), delivery of synthetic (micro- or macro-sphere embolisation) or autologous clots (thromboembolisation), transcranial vessel illumination following photosensitive dye injection (photothrombosis), and stereotactic injection of a potent vasoconstrictor (Endothelin-1) (Fluri et al., 2015; Hermann et al., 2019; Kumar et al., 2016). Of these methods, intraluminal MCAO is the most common technique applied for ischemic stroke induction in murine models.
First introduced into mice in 1993 by Chan et al. (1993), the intraluminal MCAO procedure induces a proximal large vessel occlusion in mice, through placement of a coated monofilament tip at the MCA origin. The external carotid artery (ECA) is permanently ligated, after which the partially-coated monofilament is inserted and coursed proximally to the common carotid artery (CCA) bifurcation, before being introduced into the ICA. The coated tip of the monofilament is advanced to the origin of the MCA and secured for the duration of the occlusion. Reduction of blood flow into the MCA is confirmed using Laser Doppler Flowmetry (LDF) (40-70% reduction). Adjustable variables that alter stroke severity and distribution include monofilament composition (e.g., nylon) and diameter (e.g., 3-0), monofilament tip coating material (e.g., silicone), insertion length of the monofilament (e.g., 8 mm), duration of surgery (e.g., 45 min), and duration of occlusion (e.g., 30 min) (Engel et al., 2011; Fluri et al., 2015; Lee et al., 2014). Though this model allows for permanent occlusion of the MCA, transient MCAO (tMCAO) is achieved by retracting the monofilament tip to allow for reperfusion, and is thus more clinically relevant. Additional advantages of this model are its reproducibility, regarding both infarct volume and cognitive/functional deficits, and the fact that a craniotomy is not required. tMCAO also produces an ischemic core and penumbral region, which facilitates the study of neuronal death, neuroinflammation, and blood-brain-barrier breakdown, as well as testing of therapies to rescue the penumbra.
Our group has long used the intraluminal tMCAO model of ischemic stroke induction (Khanna et al., 2017; Rink et al., 2017; Sen et al., 2017; Balch et al., 2021; Lemmerman et al., 2021). Limitations to this model include larger infarction compared to human strokes and compromised hypothalamic regulation of body temperature, which is not typically present in humans and complicates survivability of murine models (Carmichael, 2005). Additionally, distal ligation of the ECA removes blood flow to masticatory muscles, which can further reduce eating in an animal facing significant weight loss (Dittmar et al., 2003). Despite these limitations, MCAO is well-established and widely accepted for murine ischemic stroke induction in preclinical research (Fluri et al., 2015). In conjunction with a dedicated small animal surgeon, our group has spent over seven years refining the tMCAO approach, to address the limitations related to food/water intake, weight loss, and mortality. Our refined protocol for surgery and post-operative care yields successful MCA-territory infarction, while enhancing reproducibility and animal survivability. Here, we provide a detailed protocol for surgical induction of unilateral transient ischemic stroke using our refined intraluminal thread model of transient unilateral MCAO.
Materials and Reagents
Silicone Rubber-Coated Monofilament (Doccol, catalog number: 602323PK10)
Note: Monofilament size should be selected considering the weight of mice used in the study. The specific catalog number provided is suitable for animals with body weight in the range 30 ± 5 grams, as per the manufacturer.
6-0 Spool Black Braided Silk Sutures (HOSPEQ, catalog number: sp114)
6-0, P-10 Braided Polyester Absorbable Sutures (Henry Schein, Polysorb, catalog number: 2946794)
6-0, C-22 Black Braided Silk Sutures (Henry Schein, catalog number: 101-2636)
Vet Bond Tissue Adhesive (Fisher Scientific, catalog number: 15672)
Surgical Tape (3M, catalog number: 1527-0)
Cotton Tip Applicator (McKesson, Q-Tip, catalog number: 785468)
Surgical Drapes (SAI Infusion Technologies, catalog number: PSS-SD5)
Note: To provide an increased view, the surgical drapes were removed prior to images being acquired for this protocol.
Isoflurane (Primal Health Care, catalog number: NDC 66794-017-10)
Artificial tear ointment (Henry Schein, catalog number: 1338333)
Chlorhexidine (Aspen, catalog number: NDC 46066-141-01)
0.9% sodium chloride solution (Saline) (Henry Shein, catalog number: 1047098)
Ethanol, 200 Proof (100%) (Decon Labs, catalog number: 2701)
70% ethanol solution (see Recipes)
Equipment
Dumont #4 forceps (Fine Science Tools, catalog number: 11294-00)
Dumont #5 forceps 45° Inox tip (Roboz, catalog number: RS-5005)
Graefe curved and serrated forceps (×2) (Fine Science Tools, catalog number: 11051-10)
Moria Iris forceps (×2) (Fine Science Tools, catalog number: 11370-31)
Extra Fine Bonn (Iris) Scissors (Fine Science Tools, catalog number: 14084-08)
Tenotomy scissors (Fine Science Tools, catalog number: 14066-11)
Vannas Spring scissors 3mm cutting edge (Fine Science Tools, catalog number: 15000-00)
AutoClip Applier (Fine Science Tools, catalog number: 12020-09)
AutoClips (Fine Science Tools, catalog number: 12022-09)
AutoClip Remover (Fine Science Tools, catalog number: 12023-00)
Castroviejo needle Holder-Locking (Roboz, catalog number: RS-6416)
Micro clip curved (Roboz, catalog number: RS-5433)
Micro clip straight (Roboz, catalog number: RS-5424)
Mirco clip applying forceps (Roboz, catalog number: RS-5410)
Bipolar Coagulator System (Accurate Surgical, Polarmate, catalog number: AC1905)
Bipolar Forceps (Accurate Surgical, Adson, catalog number: ASSI.BPNS12723)
Laser Doppler System (Moor Instruments, catalog number: MOORVMS-LDF1-HP)
Optic Fiber (Moor Instruments, catalog number: POF500)
Slide Warmer With Temperature Control (4MD Medical, catalog number: CASCXH-2001)
Somnosuite Low-Flow Anesthesia System (Kent Scientific, catalog number: n/a)
Induction Chamber (Kent Scientific, catalog number: Somno-0705)
Warming Pad (Kent Scientific, catalog number: RT-0501)
Electric Razor with Vacuum (Remmington, catalog number: VPG-6530)
Microscope with Foot Pedals (Leica, catalog number: Wild M691)
Procedure
文章信息
版权信息
© 2022 The Authors; exclusive licensee Bio-protocol LLC.
如何引用
Readers should cite both the Bio-protocol article and the original research article where this protocol was used:
- Lemmerman, L. R., Harris, H. N., Balch, M. H. H., Rincon-Benavides, M. A., Higuita-Castro, N., Arnold, W. D. and Gallego-Perez, D. (2022). Transient Middle Cerebral Artery Occlusion with an Intraluminal Suture Enables Reproducible Induction of Ischemic Stroke in Mice. Bio-protocol 12(3): e4305. DOI: 10.21769/BioProtoc.4305.
- Lemmerman, L. R., Balch, M. H. H., Moore, J. T., Alzate-Correa, D., Rincon-Benavides, M. A., Salazar-Puerta, A., Gnyawali, S., Harris, H. N., Lawrence, W., Ortega-Pineda, L., et al. (2021). Nanotransfection-based vasculogenic cell reprogramming drives functional recovery in a mouse model of ischemic stroke. Sci Adv 7(12): eabd4735.
分类
神经科学 > 神经系统疾病 > 脑卒中
您对这篇实验方法有问题吗?
在此处发布您的问题,我们将邀请本文作者来回答。同时,我们会将您的问题发布到Bio-protocol Exchange,以便寻求社区成员的帮助。