

COVID-19 Sample Pooling: From RNA Extraction to Quantitative Real-time RT-PCR
COVID-19样本汇集:从RNA提取到实时定量RT-PCR
(*contributed equally to this work) 发布: 2021年05月05日第11卷第9期 DOI: 10.21769/BioProtoc.4005 浏览次数: 9312
评审: Alessandro DidonnaVaibhav B. ShahRan Chen
参见作者原研究论文
The authors used this protocol in:

Aug 2020
Advertisement












Abstract
The COVID-19 pandemic requires mass screening to identify those infected for isolation and quarantine. Individually screening large populations for the novel pathogen, Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), is costly and requires a lot of resources. Sample pooling methods improve the efficiency of mass screening and consume less reagents by increasing the capacity of testing and reducing the number of experiments performed, and are therefore especially suitable for under-developed countries with limited resources. Here, we propose a simple, reliable pooling strategy for COVID-19 testing using clinical nasopharyngeal (NP) and/or oropharyngeal (OP) swabs. The strategy includes the pooling of 10 NP/OP swabs for extraction and subsequent testing via quantitative real-time reverse transcription polymerase chain reaction (RT-qPCR), and may also be applied to the screening of other pathogens.
Keywords: COVID-19 (2019冠状病毒病)Background
The coronavirus disease (COVID-19) pandemic has resulted in significant socioeconomic and public health burden in affected countries worldwide. The unprecedented spread of the disease has placed healthcare systems under considerable pressure, particularly in efforts to detect cases as efficiently as possible, contain the disease, and treat cases in a timely manner. Disease surveillance and the confirmation of positive COVID-19 cases has also mostly relied upon quantitative real-time reverse transcription polymerase chain reaction (RT-qPCR) of nasopharyngeal/oropharyngeal (NP/OP) swab specimens for the detection of the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) following WHO guidelines (Corman et al., 2020). However, the RT-qPCR testing capacity can be highly variable, particularly in rural areas, where primary healthcare facilities may not have trained personnel or the necessary equipment and facilities to carry out confirmatory testing. Hence, samples are sent to centralized facilities, which in turn are met with an overwhelmingly high demand for testing. As COVID-19 cases continue to rise, these laboratories have begun to face a backlog of pending tests and rising turnaround times that affect the clinical utility of results and timely surveillance of populations at the greatest risk.
In efforts to increase the cost-effectiveness and capacity of COVID-19 screening, we developed a pooling strategy during nucleic acid extraction without a reduction in the sensitivity of RT-qPCR (Lim et al., 2020). The pooling of clinical samples has previously been employed for the screening of the human immunodeficiency virus (HIV), hepatitits C virus (HCV) (Hourfar et al., 2008), influenza viruses (Pilcher et al., 2005; Sullivan et al., 2011), and during the COVID-19 pandemic, SARS-CoV-2 (Lim et al., 2020). This method has been demonstrated to be cost-effective by allowing an increase in the viral detection capacity for mass screening while maintaining testing accuracy (Abdalhamid et al., 2020). Pooled testing for RT-qPCR has been frequently utilized (Hogan et al., 2020; Lohse et al., 2020), unlike the strategy described in this paper, where we pool samples during nucleic acid extraction prior to performing RT-qPCR. This method has been evaluated as an effective approach in recent studies (Garg et al., 2020; Wacharapluesadee et al., 2020), where in a similar fashion, NP/OP swab samples were pooled in Viral Transport Medium (VTM) for extraction. Findings by Yelin et al., (2020) suggest that even in pools of up to 32 samples, one positive sample could be detected.
Pooling during the extraction stage provides additional reductions in testing costs and workload. Using the strategy described in this protocol leads to a 9-fold reduction in the number of nucleic acid extractions and RT-qPCR reactions required (Lim et al., 2020). For laboratories conducting screening for SARS-CoV-2, the pooled testing strategy used in this protocol does not introduce any significant changes to the current testing workflow and may be incorporated into routine procedures. We note that the optimal pool size will be dependent upon, among others, the prevalence of COVID-19, the objective of the testing strategy, and the resources available to the testing facility; therefore, it is recommended that laboratories account for these differences when adopting this strategy.
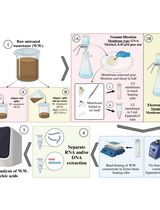
Thus, in this paper, we aim to provide a step-by-step protocol that details the pooling strategy for the screening of SARS-CoV-2. The strategy involves the pooling of 10 NP/OP swabs for extraction and subsequent testing by RT-qPCR. Implementing such a pooling strategy can minimize the costs incurred and the reagents utilized, while simultaneously reducing turnaround times for the rapid identification and isolation of positive COVID-19 cases. This protocol may also be applied to other pathogens that are screened using similar techniques, and would be particularly useful for the community screening of large groups in resource-poor settings and/or where the prevalence of infection is low.
Materials and Reagents
Personal protective equipment (PPE) appropriate for working with SARS-CoV-2
0.2 ml low-profile PCR tube strips with caps (Bio-Rad, catalog numbers: TLS0851 and TCS0903)
1.5 ml microcentrifuge tubes (Axygen, catalog number: MCT-150-C-S)
0.5-10 µl, 0.5-50 µl, 1-200 µl, 100-1,000 µl filtered pipette tips (Axygen, catalog numbers: TF-400-R-S, TF-50-R-S , TF-200-R-S, TF-1005-WB-R-S)
Geneaid Viral Nucleic Acid Extraction Kit (Geneaid Biotech, catalog number: VR300)
Qiagen DNeasy Blood and Tissue Kit (Qiagen, catalog number: 69506)
SuperScriptTM III One-Step RT-PCR System with PlatinumTM Taq DNA Polymerase (Invitrogen, catalog number: 12574-026) (aliquot and store at -20°C)
DNase- and RNase-free water (Integrated DNA Technologies, catalog number: 11-05-01-04) (aliquot into clean 1.5-ml microcentrifuge tubes)
Primers for SARS-CoV-2 (Integrated DNA Technologies) (Table 1)
Table 1. Primers and probes targerting RNA-dependent RNA polymerase (RdRP), SARS-CoV-2 detectiona
Catalog number Oligonucleotide Sequenceb CV001 RdRp_SARSr-F 5’-GTGARATGGTCATGTGTGGCGG-3’ CV002 RdRp_SARSr-R 5’-CARATGTTAAASACACTATTAGCATA-3’ CV101 RdRP_SARSr-P1 5’-FAM-CCAGGTGGWACRTCATCMGGTGATGC-BBQ-3’ CV102 RdRp_SARSr-P2 5’-FAM-CAGGTGGAACCTCATCAGGAGATGC-BBQ-3’ a Oligonucleotide sequences were adapted from the WHO-Charité protocol (Corman et al., 2020).
b W is A/T; R is G/A; M is A/C; S is G/C. FAM: 6-carboxyfluorescein; BBQ: blackberry quencher.
Primer mix (see Recipes)
Equipment
1 µl-10 µl, 10 µl-100 µl, 20 µl-200 µl, 100 µl-1,000 µl micropipettors (Eppendorf, catalog numbers: 3123000020, 3123000047, 3123000055, 3123000063)
CFX96 RealTime System (Bio-Rad, model: C1000 touch)
Thermo Aluminium Bath (Fine PCR, model: ALB128) to be used with the Qiagen DNeasy Blood and Tissue Kit
Centrifuge 5425 (Eppenddorf, catalog number: 5405000417)
Procedure
文章信息
版权信息
© 2021 The Authors; exclusive licensee Bio-protocol LLC.
如何引用
Voon, K., Johari, N. A., Lim, K. L., Wong, S. T., Khaw, L. T., Wong, S. F., Chan, E. W. L., Chan, K. K., Tan, B. K., Ramzi, N. H., Lim, P. K. C. and Sulaiman, L. H. (2021). COVID-19 Sample Pooling: From RNA Extraction to Quantitative Real-time RT-PCR. Bio-protocol 11(9): e4005. DOI: 10.21769/BioProtoc.4005.
分类
微生物学 > 病原体检测 > PCR
生物科学 > 微生物学
生物化学 > 病毒
您对这篇实验方法有问题吗?
在此处发布您的问题,我们将邀请本文作者来回答。同时,我们会将您的问题发布到Bio-protocol Exchange,以便寻求社区成员的帮助。